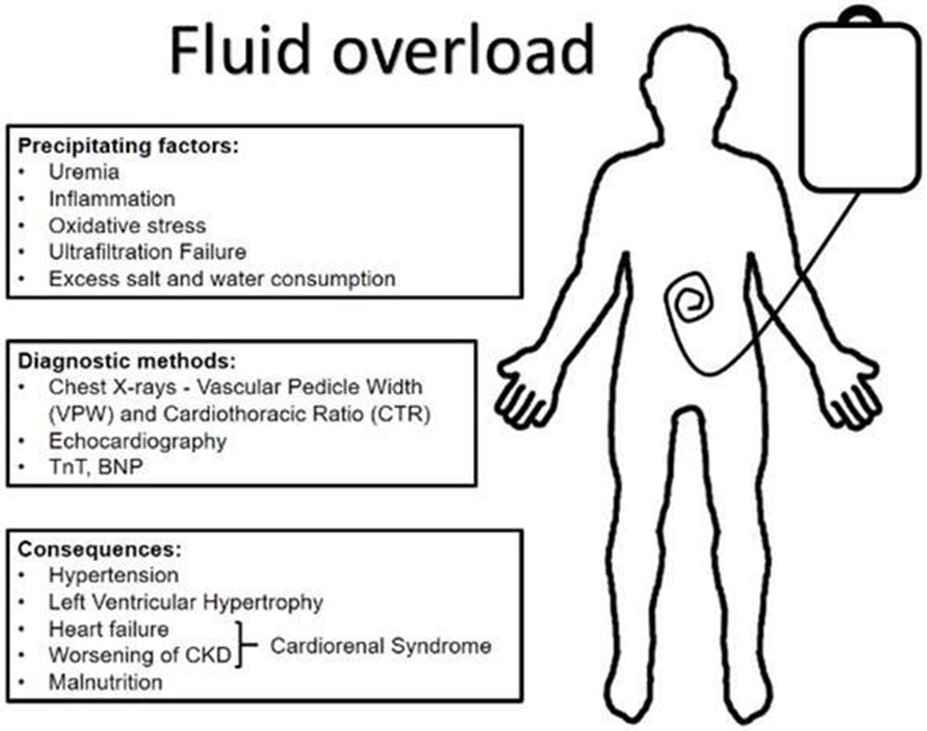
A client is receiving IV fluids at 150 mL/hr. Which of the following findings indicates that the client is experiencing fluid overload?
Oliguria
Bradycardia
Dyspnea
Poor skin turgor
The Correct Answer is C
- A. Oliguria. This is incorrect because oliguria, or decreased urine output, is a sign of fluid volume deficit, not fluid volume overload.
- B. Bradycardia. This is incorrect because bradycardia, or slow heart rate, is not a typical sign of fluid volume overload, unless the client has a cardiac condition that affects the heart's response to fluid overload.
- C. Dyspnea. This is correct because dyspnea, or difficulty breathing, is a common sign of fluid volume overload, as excess fluid accumulates in the lungs and impairs gas exchange.
- D. Poor skin turgor. This is incorrect because poor skin turgor, or decreased elasticity of the skin, is a sign of dehydration, not fluid volume overload.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
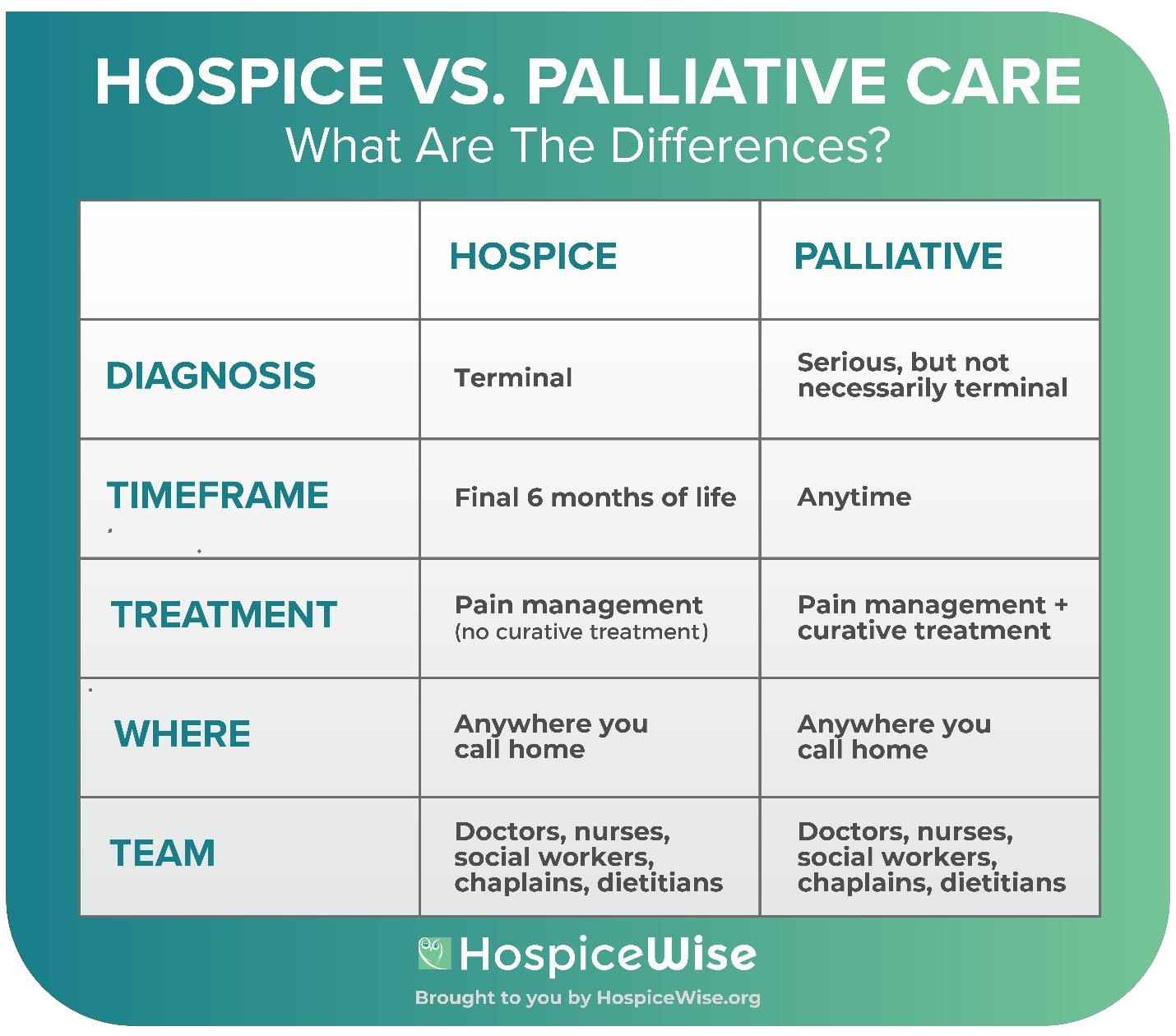
Hospice care includes bereavement support for the family for up to a year after the client's death.
- B is incorrect because the hospice nurse does not administer pain medication, but rather teaches the family how to manage the client's pain at home.
- C is incorrect because respite care is one of the services that hospice provides to allow the family to take a break from caregiving.
- D is incorrect because hospice care does not aim to prolong life, but rather to provide comfort and quality of life for the client and the family.
Correct Answer is C
Explanation
- A. Incorrect. Evaluating dietary intake requires nursing judgment and knowledge of nutrition and eating disorders. This task should not be delegated to an AP.
- B. Incorrect. Measuring vital signs of a postoperative client requires nursing assessment and monitoring for complications. This task should not be delegated to an AP.
- C. Correct. Arranging the lunch tray for a client who has a hip fracture is a routine task that does not require nursing skills or judgment. This task can be delegated to an AP.
- D. Incorrect. Assessing I&O for a client who is receiving dialysis requires nursing knowledge of fluid and electrolyte balance and renal function. This task should not be delegated to an AP.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today