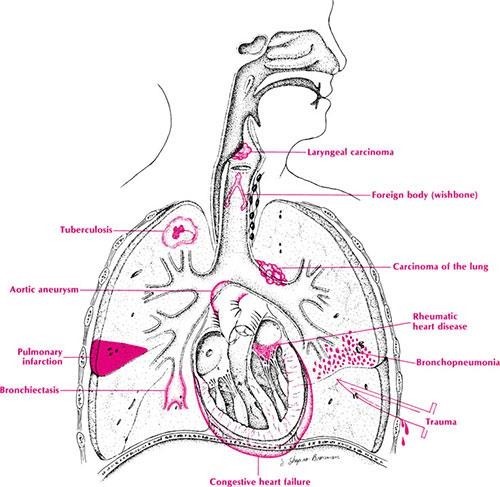
A client is admitted with shortness of breath and hemoptysis. After several tests, the healthcare provider informs the client that the medical diagnosis is stage 4 breast cancer. The client tells the nurse about the decision not to inform the family about the diagnosis. Which intervention should the nurse implement?
Notify the health department of the client's condition.
Advise the client to weigh all possible outcomes prior to the decision.
Suggest to the family the value of genetic screening.
Explain that the family has a right to know of potential health problems.
Explain that the family has a right to know of potential health problems.
The Correct Answer is B
A) This intervention is not appropriate because it violates the client's privacy and confidentiality. The health department does not need to be notified of the client's condition, as breast cancer is not a communicable disease or a public health threat. The nurse should respect the client's wishes and only share information with authorized persons or agencies.
B) This intervention is appropriate because it respects the client's autonomy and encourages informed decision-making. The nurse should advise the client to consider the benefits and risks of disclosing or withholding the diagnosis from the family, and how it may affect their relationships and support systems. The nurse should also provide relevant information and resources to help the client make an informed choice.
C) This intervention is not appropriate because it contradicts the client's decision and may cause confusion or distress for the family. The nurse should not suggest genetic screening to the family without the client's consent, as this may imply that they are at risk of developing breast cancer or other genetic disorders. The nurse should also avoid giving unsolicited advice or opinions that may interfere with the client's autonomy.
D) This intervention is not appropriate because it imposes the nurse's values and beliefs on the client. The nurse should not explain that the family has a right to know of potential health problems, as this may imply that the client is wrong or selfish for withholding the diagnosis. The nurse should acknowledge and respect the client's perspective and preferences, and support them in coping with their condition.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: The ability to update the equipment each year may be desirable, but not the most important question to consider. Updating the equipment may incur additional costs and may not be necessary or feasible depending on the type and function of the equipment.
Choice B Reason: The number of departments that can use the equipment is the most important question to
consider, as it reflects the potential impact and benefit of the equipment for the organization. The more departments that can use the equipment, the more efficient and cost-effective it will be.
Choice C Reason: The cost of equipment is an important question to consider, but not the most important one. The cost of equipment should be compared with the expected benefits and outcomes of using the equipment, not just in terms of monetary value, but also in terms of quality of care and patient satisfaction.
Choice D Reason: The need for annual repair is an important question to consider, but not the most important one. The need for annual repair may indicate the reliability and durability of the equipment, but it may also depend on the frequency and intensity of use, and the availability and accessibility of maintenance services.
Correct Answer is ["B","C"]
Explanation
Choice A Reason: Identifying locations of skin lesions on a newly admitted client is a nursing assessment that requires clinical judgment and cannot be delegated to the UAP.
Choice B Reason: Emptying the ostomy bag for a client with a temporary colostomy is a routine task that does not require clinical judgment and can be delegated to the UAP.
Choice C Reason: Providing a complete bed bath for a comatose client is a routine task that does not require clinical judgment and can be delegated to the UAP.
Choice D Reason: Performing foot care including toenail trimming and heel care is a nursing intervention that requires clinical judgment and cannot be delegated to the UAP. The UAP may cause injury or infection to the client's feet, especially if the client has diabetes or peripheral vascular disease.
Choice E Reason: Giving mouth care to an elderly client who has a tracheostomy is a nursing intervention that requires clinical judgment and cannot be delegated to the UAP. The UAP may cause trauma or aspiration to the client's trachea, especially if the client has poor oral hygiene or respiratory secretions.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today