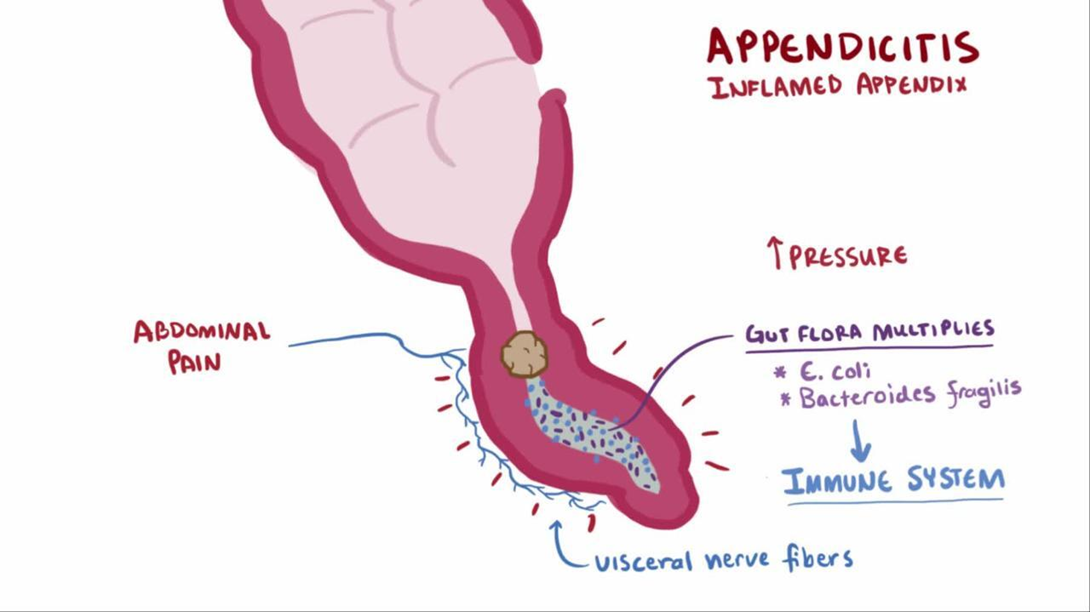
While completing a health assessment for a young adult female with acute appendicitis, the client informs the nurse that there is a chance that she may be pregnant. The operating team is preparing to take the client to surgery. Which intervention should the nurse implement immediately?
Perform a bedside pregnancy test.
Continue with surgery as scheduled.
Calculate gestation from last menstrual cycle.
Notify the surgical team to cancel the surgery.
The Correct Answer is A
Choice A reason: This is correct because performing a bedside pregnancy test is the intervention that should be implemented immediately by the nurse. This is to confirm or rule out pregnancy and inform the surgical team of any possible risks or complications that may affect the client or the fetus.
Choice B reason: This is incorrect because continuing with surgery as scheduled is not an appropriate intervention without verifying the pregnancy status of the client. Surgery may pose serious threats to both maternal and fetal health, such as bleeding, infection, anesthesia complications, or miscarriage.
Choice C reason: This is incorrect because calculating gestation from last menstrual cycle is not an accurate or reliable method of determining pregnancy. The menstrual cycle can vary widely among women and may be affected by various factors such as stress, illness, or medication.
Choice D reason: This is incorrect because notifying the surgical team to cancel the surgery is not a necessary intervention unless pregnancy is confirmed. Appendicitis is a medical emergency that requires prompt surgical treatment to prevent rupture, peritonitis, or sepsis.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A: A headache rated at 0 on 0 to 10 scale is not a specific indicator of the effectiveness of an antihistamine. A headache may be caused by other factors, such as dehydration, stress, or sinus congestion.
Choice B: Oxygen saturation level of 99% is a normal finding and does not reflect the effect of an antihistamine. Oxygen saturation measures the amount of oxygen in the blood and can be affected by respiratory conditions, altitude, or smoking.
Choice C: Ambulating easily without vertigo is a sign that the antihistamine is effective. Vertigo is a common symptom of Ménière's disease, which is a disorder of the inner ear that causes episodes of spinning sensation, hearing loss, and tinnitus. Antihistamines can help reduce the fluid buildup in the inner ear and relieve vertigo.
Choice D: Blood pressure of 120/80 mm Hg is a normal finding and does not indicate the effect of an antihistamine. Blood pressure measures the force of blood against the walls of the arteries and can be influenced by factors such as heart rate, cardiac output, blood volume, and vascular resistance.
Correct Answer is C
Explanation
Choice A reason: An abdominal catheter is used for peritoneal dialysis, not hemodialysis. Hemodialysis requires access to a large blood vessel, usually in the arm or leg.
Choice B reason: Routine medications may need to be adjusted or avoided before or after hemodialysis, depending on their effects on blood pressure, fluid balance, and electrolytes.
Choice C reason: Insulin dosage may need to be reduced during hemodialysis because insulin is removed by the dialyzer and blood glucose levels may drop. This is the correct statement to include in client education.
Choice D reason: Potassium-rich foods should be limited in the diet of clients with chronic kidney disease and hemodialysis, because potassium can build up in the blood and cause cardiac arrhythmias.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today