The practical nurse (PN) is charting vital signs on a hand-writen flow sheet and realizes that an error has been made. What should the PN do to rectify this error?
Obliterate the entry and insert the correct information
Draw one line through the entry and insert the correct information
Chart the correct information in the next column.
Notify the charge nurse that the entry needs to be revised
The Correct Answer is B
This is the correct way to correct an error on a hand-writen chart, according to the legal and ethical principles of documentation. The PN should also initial and date the correction.
Obliterating the entry or charting in the next column can create confusion and suspicion of tampering with the records. Notifying the charge nurse is not necessary unless the error has serious implications for the client's care or safety
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","D"]
Explanation
The correct answers are Choice B and D:
Choice B: Report the appearance of the dressing to the charge nurse,
Choice D: Compress the drainage device before closing the tab.
Choice A rationale:
Documenting the appearance of the wound as inflamed is not appropriate. As a practical nurse, the immediate concern is to take action and report any concerning findings to the appropriate healthcare provider rather than just documenting it.
Choice B rationale:
Reporting the appearance of the dressing to the charge nurse is essential. The charge nurse or a more experienced healthcare provider needs to be informed of any abnormal findings or signs of infection for further evaluation and appropriate intervention.
Choice C rationale:
Removing the drainage device and applying a pressure dressing is not within the scope of practice for a practical nurse. These actions require a higher level of expertise and are typically performed by a registered nurse or healthcare provider.
Choice D rationale:
Compressing the drainage device before closing the tab is a correct action. This helps to ensure that the device is functioning properly, and there are no leaks or obstructions in the drainage system.
Choice E rationale:
Clamping the drainage tubing for the next four hours is not recommended unless specifically ordered by a healthcare provider. Clamping the drainage tubing without appropriate orders may disrupt the normal drainage process and cause complications.
Correct Answer is A
Explanation
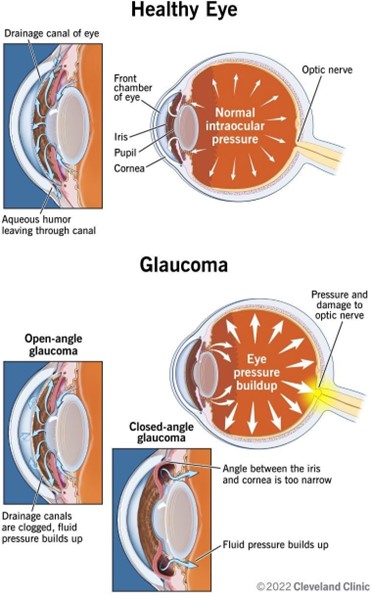
Glaucoma is a group of eye diseases that damage the optic nerve and cause vision loss. It is often associated with increased intraocular pressure, which can compress the nerve fibers and reduce blood flow to the retina. The most common type of glaucoma, open-angle glaucoma, causes gradual loss of peripheral vision.
The other options are not correct because:
A. Macular edema is a condition that causes swelling and fluid accumulation in the macula, the central part of the retina that is responsible for sharp and detailed vision. It can cause blurred or distorted vision, but it does not affect the optic nerve or the peripheral vision.
B. Cataract is a condition that causes clouding of the lens, which is the transparent structure that focuses light onto the retina. It can cause blurred, dim, or yellowed vision, but it does not affect the optic nerve or the intraocular pressure.
C. Diabetic retinopathy is a complication of diabetes that damages the blood vessels in the retina and causes bleeding, leakage, or scarring. It can cause blurred, fluctuating, or darkened vision, but it does not affect the optic nerve or the intraocular pressure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today