The practical nurse (PN) reviews the history of an older adult who is newly admitted to a long-term care facility. Which factor in the resident's history should the PN consider the most likely to increase the client's risk for falls?
Ankle ulcer that is healing slowly.
History of alcohol abuse and cigarete smoking.
Recent weight gain of twenty pounds.
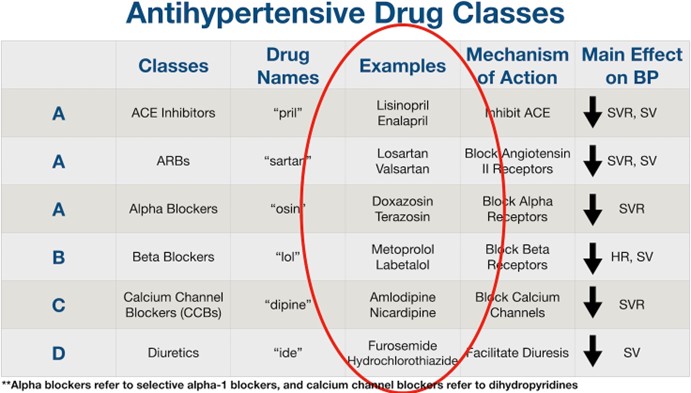
Newly prescribed antihypertensive medication.
The Correct Answer is D
This is the factor that the PN should consider the most likely to increase the client's risk for falls because it can cause orthostatic hypotension, dizziness, or fainting, especially when the client changes position or gets up from bed or a chair. The PN should monitor the client's blood pressure and pulse before and after administering the medication and assist the client with ambulation and transfers.
A. An ankle ulcer that is healing slowly is not a major risk factor for falls and may not affect the client's mobility or balance.
B. History of alcohol abuse and cigarette smoking is not a major risk factor for falls unless the client is currently intoxicated or has a chronic lung disease that impairs oxygenation or cognition.
C. Recent weight gain of twenty pounds is not a major risk factor for falls unless it causes joint pain, edema, or difficulty moving.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
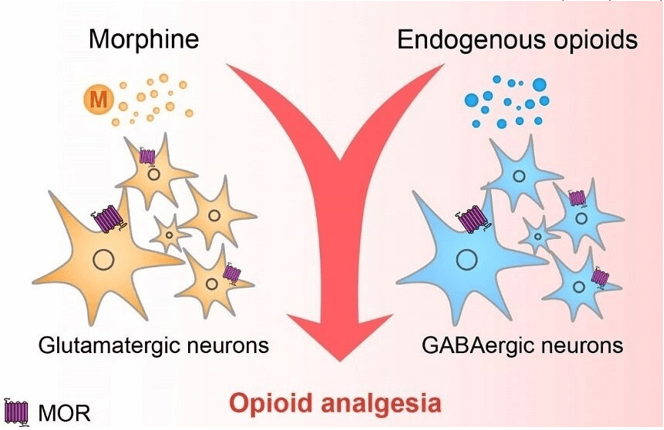
Correct Answer is B
Explanation
This is the best action for the PN to use in assisting this client to deal with his pain because it provides a non- pharmacological method of pain relief that can enhance the effect of the opioid analgesic. Slow, rhythmic breathing can help the client relax, distract from the pain, and increase oxygenation and blood flow.
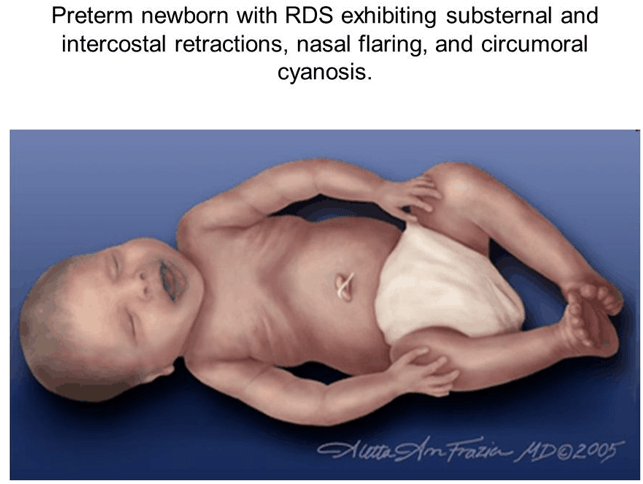
Correct Answer is A
Explanation
Circumoral cyanosis is a bluish discoloration around the mouth that indicates inadequate oxygenation. It is an abnormal finding in a full-term newborn and requires immediate assessment and intervention by the PN.
The other options are not correct because:
- A positive Babinski's reflex is a normal finding in newborns that indicates intact neurological function. It is elicited by stroking the sole of the foot and observing the fanning of the toes.
- A negative Ortolani's sign is a normal finding in newborns that indicates no hip dislocation or dysplasia. It is elicited by abducting the hips and feeling for any clicking or clunking sensation.
- A large sacral "stork bite" is a common benign birthmark that appears as a reddish patch on the lower back or nape of the neck. It usually fades within the first year of life and does not require any treatment.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today