The nurse working in an ophthalmology clinic is preparing to assess a patient's near vision. Which piece of equipment would the nurse use for this assessment?
Ophthalmoscope
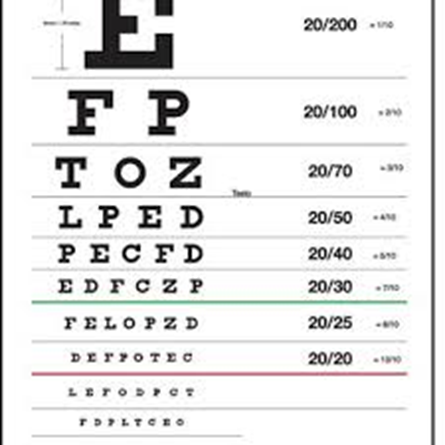
Snellen Chart
Magazine
Penlight
The Correct Answer is B
Choice A Reason:
An ophthalmoscope is primarily used for examining the interior structures of the eye, such as the retina, and is not typically used for assessing near vision. It provides a view of the fundus of the eye, which is essential for diagnosing various eye conditions but does not directly assess a patient's reading or close-up vision.
Choice B Reason:
The Snellen Chart is traditionally used to measure distance visual acuity and would not be the first choice for assessing near vision. However, there are versions of the Snellen Chart or similar charts designed for near vision assessment, typically held at a reading distance of about 14 inches from the patient. These charts have rows of letters or symbols that decrease in size and are used to determine the smallest print size a person can read.
Choice C Reason:
A magazine can be a practical tool for assessing near vision informally, as it contains various sizes of print and is a good representation of everyday reading material. The nurse can ask the patient to read a specific paragraph to observe their ability to see and comprehend text at a close distance.
Choice D Reason:
A penlight is not used for assessing near vision. It is typically used to assess the pupillary light reflex or to illuminate specific areas of the eye during an examination. The penlight helps to evaluate the response of the pupils to light but does not measure the patient's ability to read or see objects up close.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice a reason:
Immunization schedules are typically considered a part of primary prevention. They are intended to prevent diseases before they occur by using vaccines to provide immunity against infections.
Choice b reason:
Regular mammogram screenings are a form of secondary prevention. They are used to detect breast cancer lesions early before symptoms appear, which can lead to more effective treatment and better outcomes.
Choice c reason:
The consistent use of seat belts is a primary prevention strategy. It is a proactive measure to prevent injuries in the event of a motor vehicle accident.
Choice d reason:
Annual vision examinations can be considered part of secondary prevention if they are used to detect vision problems or eye diseases in their early stages. However, they can also be seen as primary prevention because they help maintain and protect eye health before issues arise.
Correct Answer is B
Explanation
Choice a reason:
Draping body areas that are not being assessed is important for maintaining the client's privacy and comfort, but it is not the highest priority when dealing with a client with generalized muscle weakness. The primary concern is to prevent further strain or injury during the examination.
Choice b reason:
Limiting position changes as much as possible is the priority when examining a client with generalized muscle weakness. Frequent or unnecessary movements can cause fatigue, discomfort, and may even be unsafe if the client has severely compromised muscle strength. The nurse should plan the examination to minimize the number of times the client needs to change positions.
Choice c reason:
Hand-washing throughout the exam is a standard practice to prevent the spread of infection. While it is crucial for both the client's and the nurse's safety, in the context of a client with generalized muscle weakness, the priority is to conduct the exam in a way that does not exacerbate the client's condition.
Choice d reason:
Using alcohol swabs to clean the stethoscope before and after the exam is also a standard infection control practice. However, it is not the most immediate concern when prioritizing the steps of a physical examination for a client with muscle weakness.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today