The nurse is obtaining the client's vital signs prior to an endoscopy.
Complete the following sentence by using the list of options.
The nurse should first anticipate the need to
The Correct Answer is {"dropdown-group-1":"B","dropdown-group-2":"A"}
The nurse should first anticipate the need to withhold oral intake then assess the client's vital signs.
Given the client’s symptoms of gnawing abdominal pain, dark tarry stools (indicating possible gastrointestinal bleeding), and pain worsened by eating, withholding oral intake is crucial to prevent further irritation or complications, especially before an endoscopic procedure. This helps avoid complications such as aspiration or exacerbating gastrointestinal issues. After ensuring that oral intake is managed appropriately, the nurse should then assess the client's vital signs to monitor for signs of hemodynamic instability or further deterioration, which can provide critical information about the client's current condition and guide further interventions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["0.25"]
Explanation
To calculate the required amount of the medication, divide the desired dose (0.5 mg. by the concentration (2 mg/mL.:
0.5 mg / 2 mg/mL = 0.25 mL
Correct Answer is B
Explanation
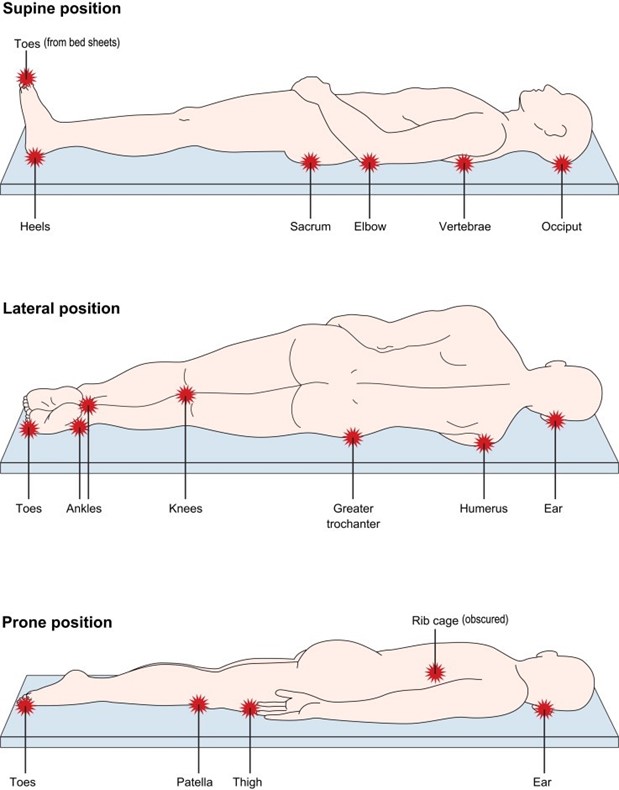
The occiput refers to the back of the head. Placing a small pillow or padding under the occiput can help relieve pressure and provide support to the client's head and neck when they are placed in the supine position.
Breasts: When in the prone position, breasts may be compressed or flattened. To relieve pressure, it may be necessary to use positioning techniques that distribute weight evenly and avoid direct pressure on the breasts, such as using cushions or foam pads to support the chest and torso.
Heels: The heels are prone to pressure ulcers when a client is lying in the supine position for extended periods. To relieve pressure, it is important to use proper heel offloading techniques, such as placing heel protectors or pillows under the lower legs to elevate the heels off the bed surface and prevent direct pressure.
Coccyx: The coccyx is the tailbone region at the base of the spine. When in the supine position, pressure on the coccyx can be relieved by using a cushion or padding under the pelvic area, specifically under the bony prominence of the coccyx, to reduce direct pressure and provide comfort.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today