The nurse is examining a client for tactile fremitus. The nurse recognizes that when examining for tactile fremitus it is important to:
Have the client breathe quickly
Palpate the chest symmetrically
Ask the client to cough
Use the bell of the stethoscope
The Correct Answer is B
A. Have the client breathe quickly:
This choice is incorrect because having the client breathe quickly is not a technique for assessing tactile fremitus. Tactile fremitus is assessed by feeling vibrations on the chest wall while the patient speaks, not during normal breathing.
B. Palpate the chest symmetrically:
This choice is correct. To assess tactile fremitus, the nurse places the palms or ulnar aspects of both hands firmly against the patient's chest while the patient speaks a phrase. The nurse should palpate the chest symmetrically to detect vibrations equally on both sides, which can help identify abnormalities in the lungs.
C. Ask the client to cough:
This choice is incorrect. Asking the client to cough is not a technique for assessing tactile fremitus. Tactile fremitus is evaluated by feeling vibrations while the patient speaks, not while coughing.
D. Use the bell of the stethoscope:
This choice is incorrect. Tactile fremitus is assessed by palpation, not auscultation with a stethoscope. Using the bell of the stethoscope is a technique for listening to low-pitched sounds, not for assessing tactile fremitus.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
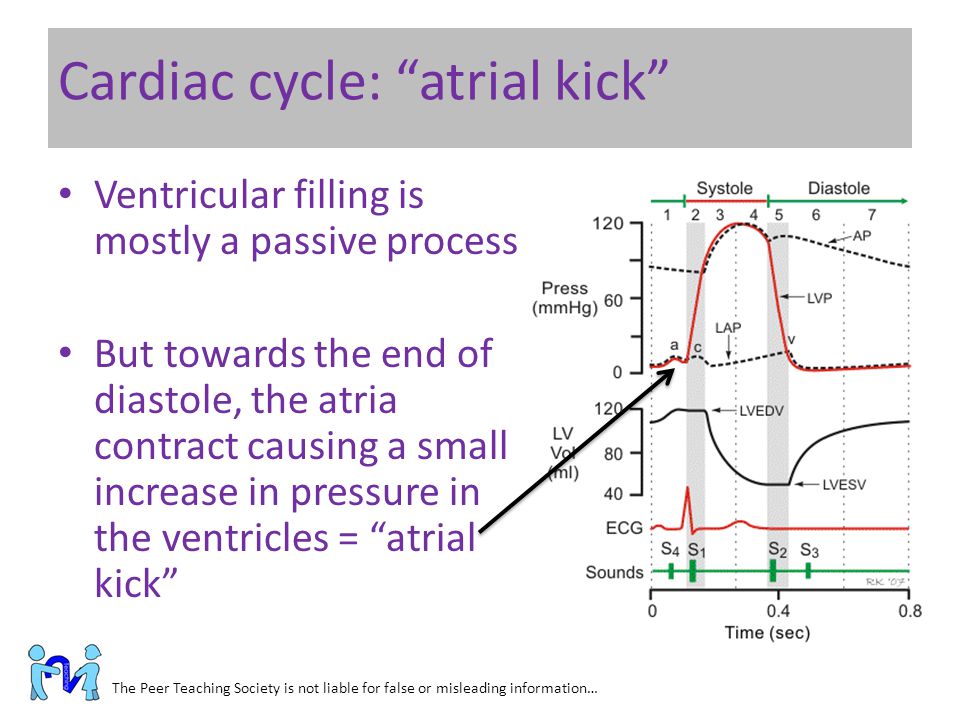
A. The atria contract toward the end of diastole and push the remaining blood into the ventricles.
This choice is correct. During atrial systole (atrial contraction), the atria contract, pushing the remaining blood into the ventricles. This additional filling of the ventricles optimizes cardiac output.
B. The atria contract during systole and attempt to push against closed valves.
This statement is incorrect. The atria do not contract during systole; they contract during diastole (atrial systole) to fill the ventricles.
C. Atrial kick is the pressure exerted against the atria as the ventricles contract during systole.
This statement is incorrect. Atrial kick refers to the atrial contraction, not the pressure exerted against the atria.
D. Contraction of the atria at the beginning of diastole can be felt as a palpitation.
This statement is not entirely accurate. A palpitation is a sensation of rapid or strong heartbeat, which might be felt during various cardiac events, not specifically during atrial contraction at the beginning of diastole.
Correct Answer is D
Explanation
A. When bronchial breath sounds are auscultated in the trachea.
Auscultating bronchial breath sounds in the trachea is a normal finding, as the trachea is close to the upper airway, and this is where bronchial sounds are normally heard. However, if these sounds are heard in the peripheral lung fields, it can indicate an abnormal condition.
B. When the client is experiencing excessive sneezing from a tree pollen allergy.
Excessive sneezing due to allergies would not typically result in increased breath sounds. Allergies may cause nasal congestion, but they don't directly lead to increased breath sounds.
C. When the client is resting in bed and not experiencing respiratory issues.
If a client is at rest and not experiencing any respiratory issues, breath sounds should typically be normal. There would be no reason to expect increased breath sounds in this scenario.
D. When the bronchial tree is obstructed by secretions.
Increased breath sounds, such as wheezing or rhonchi, can be auscultated when there is an obstruction in the bronchial tree due to secretions, narrowing of the airways, or other causes. These sounds are typically abnormal and indicate an issue with air movement through the airways.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today