The nurse administers risedronate to a client with osteoporosis at 0700. The client asks for a glass of milk to drink with the medication. Which action should the nurse take?
Instruct the client that it is necessary to take nothing but water with the medication.
Assign an unlicensed assistive personnel (UAP) to bring the client a glass of low fat milk.
Withhold the medication until the client's breakfast tray is available on the unit.
Consult with a pharmacist about scheduling the dose one hour after the client eats.
The Correct Answer is A
Choice A reason: Risedronate is a bisphosphonate that is used to treat osteoporosis by inhibiting bone resorption. It should be taken on an empty stomach with a full glass of water at least 30 minutes before any other food, beverage, or medication. This is because food, milk, and antacids can interfere with the absorption of risedronate and reduce its effectiveness.
Choice B reason: Milk contains calcium, which can bind to risedronate and prevent its absorption. Therefore, the client should not drink milk with or within 2 hours of taking risedronate.
Choice C reason: Withholding the medication until the client's breakfast tray is available is not appropriate, as it would delay the administration of risedronate and disrupt the dosing schedule. The client should take risedronate as soon as possible after waking up and before eating anything.
Choice D reason: Consulting with a pharmacist about scheduling the dose one hour after the client eats is not necessary, as risedronate should be taken at least 30 minutes before any food or beverage. Taking risedronate one hour after eating may not ensure adequate absorption of the drug.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice B reason: Epoetin alfa is a synthetic form of erythropoietin, a hormone that stimulates the production of red blood cells (RBCs) in the bone marrow. Epoetin alfa is used to treat anemia, or low RBC count, which can be caused by CKD, chemotherapy, HIV infection, or other conditions. Anemia can cause symptoms such as weakness, fatigue, shortness of breath, pale skin, and chest pain. Hemoglobin is the protein in RBCs that carries oxygen throughout the body. The normal range of hemoglobin for males is 14 to 18 g/dL (8.7 to 11.2 mmol/L). Therefore, an increase in hemoglobin from below normal to within normal indicates that epoetin alfa has been effective in increasing RBC production and improving oxygen delivery. The nurse should monitor the client's hemoglobin level regularly and adjust the dose of epoetin alfa as needed.
Choice A reason:While iron therapy supports the effectiveness of epoetin alfa by providing the necessary substrate for erythropoiesis, tolerating iron therapy is not an indicator of epoetin alfa's efficacy.
Choice C reason: Epoetin alfa is used to treat anemia associated with chronic kidney disease (CKD) by stimulating erythropoiesis (red blood cell production). The primary measure of its effectiveness is an increase in hemoglobin (Hgb) levels toward the target range. The hemoglobin level increasing to 12 g/dL (7.45 mmol/L) reflects a significant improvement from an anemic state and is within the target range for patients receiving epoetin alfa therapy (generally 10–12 g/dL). This is the most objective and definitive indicator of the medication's effectiveness.
Choice D reason: Taking concurrent iron therapy without adverse effects is not a finding that best indicates that the medication is effective, but rather a preventive measure that can reduce the risk of iron deficiency and improve the efficacy of epoetin alfa. Iron therapy refers to taking oral or intravenous iron supplements to increase iron levels in the blood. Iron therapy can cause side effects such as nausea, vomiting, constipation, diarrhea, dark stools, metallic taste, or allergic reactions. The nurse should instruct the client on how to take iron therapy safely and monitor for any adverse effects.
Correct Answer is D
Explanation
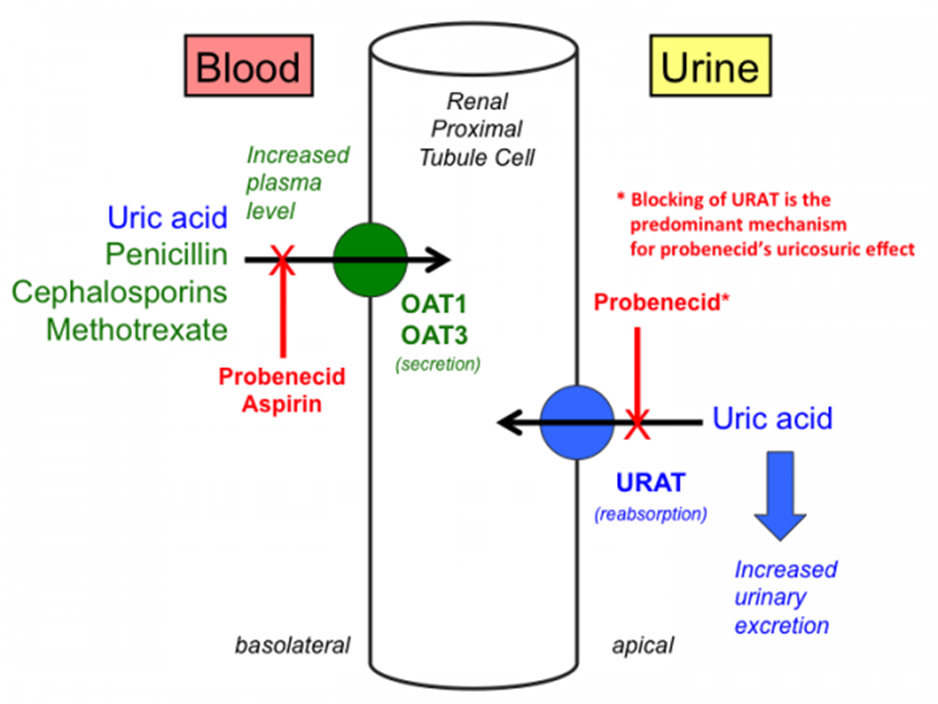
Choice D reason: Probenecid is a uricosuric drug that increases the excretion of uric acid in the urine by inhibiting its reabsorption in the kidneys. Uric acid is a waste product that results from the breakdown of purines, which are found in certain foods and drinks, such as meat, seafood, beer, and wine. Probenecid is used to treat gout, a type of arthritis that occurs when uric acid crystals accumulate in the joints and cause inflammation, pain, swelling, and stiffness. By lowering uric acid levels in the blood, probenecid can prevent gout attacks and reduce joint damage.
Choice A reason: Increasing the strength of the urine stream is not a purpose of probenecid, but rather a possible effect of some medications that relax or dilate the urinary tract muscles, such as alpha-blockers or anticholinergics. These medications can help to improve urinary flow and reduce symptoms of benign prostatic hyperplasia (BPH), or enlarged prostate gland, which can cause difficulty urinating or weak urine stream.
Choice B reason: Preventing the formation of kidney stones is not a purpose of probenecid, but rather a potential benefit of some medications that lower calcium or oxalate levels in the urine, such as thiazide diuretics or potassium citrate. These medications can help to prevent calcium oxalate stones, which are one of the most common types of kidney stones. Kidney stones are hard deposits of minerals and salts that form in the kidneys and can cause severe pain, nausea, vomiting, and blood in the urine.
Choice C reason: Decreasing pain and burning during urination is not a purpose of probenecid, but rather a desired outcome of some medications that treat urinary tract infections (UTIs), such as antibiotics or phenazopyridine. These medications can help to eliminate the bacteria that cause UTIs and relieve the discomfort and inflammation that they cause. UTIs are infections that affect the bladder, urethra, or kidneys and can cause frequent or urgent urination, pain or burning during urination, cloudy or foul-smelling urine, and fever.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today