While making rounds, the charge nurse notices that a young adult client with asthma who was admitted yesterday is sitting on the side of the bed and leaning over the bed-side table. The client is currently receiving oxygen at 2 liters/minute via nasal cannula. The client is wheezing and is using pursed lip breathing. Which intervention should the nurse implement?
Increase oxygen to 6 liters/minute.
Call for an Ambu resuscitation bag.
Instruct the client to lie back in bed.
Administer a nebulizer treatment.
The Correct Answer is D
Choice A reason: Increasing oxygen to 6 liters/minute is not an intervention that the nurse should implement, as this can worsen the bronchospasm and hypoxia by reducing the hypoxic drive and causing carbon dioxide retention. This is a contraindicated choice.
Choice B reason: Calling for an Ambu resuscitation bag is not an intervention that the nurse should implement, as this is not indicated for a client who is conscious and breathing spontaneously. This is an overreaction choice.
Choice C reason: Instructing the client to lie back in bed is not an intervention that the nurse should implement, as this can increase respiratory distress and compromise airway clearance by reducing lung expansion and increasing abdominal pressure. This is another contraindicated choice.
Choice D reason: Administering a nebulizer treatment is an intervention that the nurse should implement, as this can deliver bronchodilators and anti-inflammatory agents directly to the airways and improve ventilation and oxygenation for this client. Therefore, this is the correct choice.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice D reason: allowing time for the behavior and then redirecting the client to other activities is an effective intervention for a client with OCD who is repeatedly washing the top of the same table. OCD is a disorder characterized by recurrent and intrusive thoughts (obsessions) and repetitive and ritualistic behaviors (compulsions) that cause distress and impairment. The nurse should not interfere with or criticize the client's compulsions, as this can increase anxiety and resistance. The nurse should instead set limits on the time and place for the compulsions and gradually reduce them by offering alternative coping strategies or distractions.
Choice A reason: encouraging the client to be calm and relax for a while is not an effective intervention for a client with OCD who is repeatedly washing the top of the same table. The client may not be able to relax or stop their compulsions, as they are driven by irrational fears or beliefs that are difficult to control. The nurse should not minimize or dismiss the client's feelings, as this can make them feel misunderstood or invalidated.
Choice B reason: teaching the client thought-stopping techniques and how to refocus behaviors is not an effective intervention for a client with OCD who is repeatedly washing the top of the same table. Thought-stopping techniques are cognitive strategies that aim to interrupt or replace negative or unwanted thoughts with positive or neutral ones. However, these techniques may not work for clients with OCD, as their obsessions are often persistent and resistant to change. The nurse should not attempt to teach new skills or challenge the client's thoughts during an acute episode of compulsion, as this can increase anxiety and frustration.
Choice C reason: assisting the client to identify stimuli that precipitate the activity is not an effective intervention for a client with OCD who is repeatedly washing the top of the same table. The client may not be able to identify or avoid the triggers that cause their compulsions, as they are often internal or irrational. The nurse should not focus on finding the cause or meaning of the compulsions, as this can reinforce their significance or validity.
Correct Answer is B
Explanation
Choice A reason: Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
Choice B reason: This is the correct answer because maintaining a continuous infusion of IV fluids per prescription is essential to prevent dehydration and electrolyte imbalance in the infant. The infant may have significant fluid loss due to vomiting and poor intake.
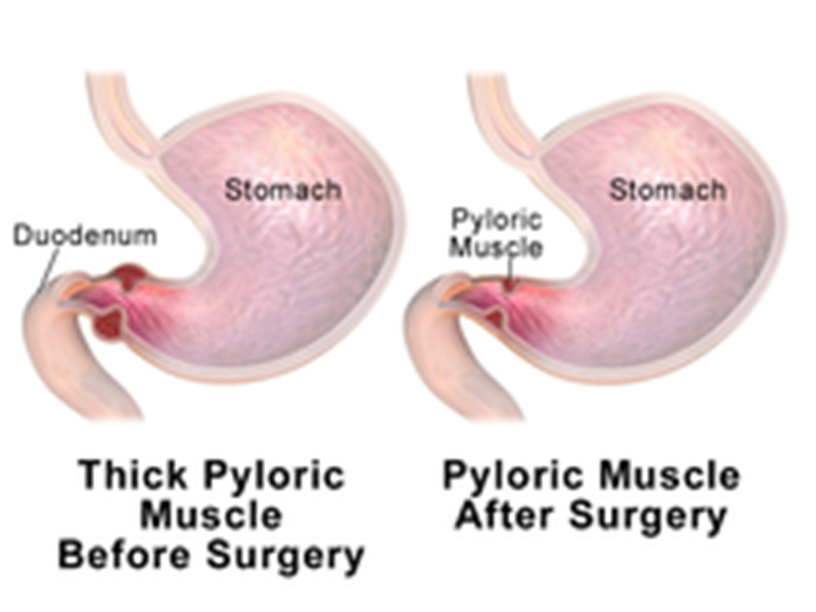
Choice C reason: Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
Choice D reason: Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today