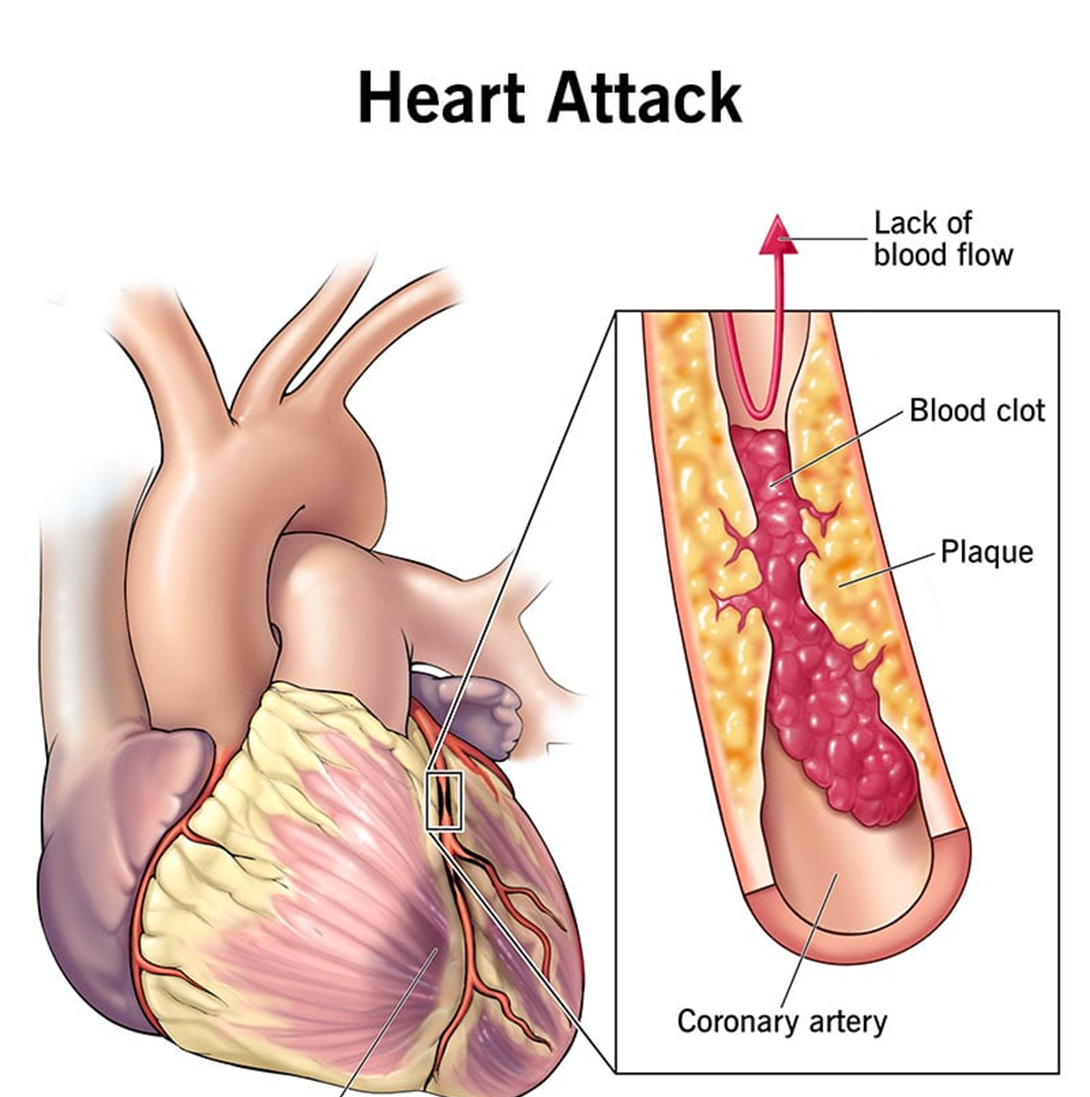
A 46-year-old male client who had a myocardial infarction (MI) 24 hours ago comes to the nurse's station fully dressed and wanting to go home. He tells
the nurse that he is feeling much better at this time. Based on this behavior, which client problem should the nurse include in the plan of care?
Ineffective coping related to denial
Emotional conflict due to stress
Deficient knowledge of MI lifestyle changes
Anxiety related to treatment plan
The Correct Answer is A
Choice A reason: This is the correct answer because ineffective coping related to denial is a likely problem for a client who had an MI 24 hours ago and wants to go home despite his condition. Denial is a defense mechanism that helps people avoid facing unpleasant or threatening realities, such as having a heart attack and needing hospitalization and treatment. The nurse should assess the client's coping skills and provide emotional support and education.
Choice B reason: Emotional conflict due to stress is not a specific problem for a client who had an MI 24 hours ago and wants to go home despite his condition. Emotional conflict is a state of having mixed or contradictory feelings about something or someone, such as family, work, or self. Stress is a response to any physical, psychological, or environmental demand that exceeds one's coping resources. The nurse should assess the client's sources of stress and conflict and help him manage them.
Choice C reason: Deficient knowledge of MI lifestyle changes is not a primary problem for a client who had an MI 24 hours ago and wants to go home despite his condition. Deficient knowledge is a state of lacking information or understanding about something, such as disease process, treatment options, or self-care measures. Lifestyle changes are modifications in one's habits or behaviors that promote health and well-being, such as diet, exercise, smoking cessation, or stress management. The nurse should assess the client's learning needs and readiness and provide appropriate education.
Choice D reason: Anxiety related to treatment plan is not an evident problem for a client who had an MI 24 hours ago and wants to go home despite his condition. Anxiety is a feeling of apprehension, worry, or fear that interferes with one's normal functioning or well-being. Treatment plan is a set of goals, interventions, and outcomes that guide the care of a client with a specific health problem, such as MI. The nurse should assess the client's level of anxiety and provide information and reassurance about his treatment plan.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: Think about reasons the episodes occur. This is not the best instruction, as it may increase the anxiety level of the client. Thinking about reasons may trigger negative thoughts, emotions, or memories that can worsen the anxiety. The nurse should teach the client to focus on coping skills rather than causes.
Choice B reason: Center attention on positive upbeat music. This is not the best instruction, as it may not be effective for all clients. Listening to positive upbeat music may help distract or soothe some clients, but it may also irritate or annoy others. The nurse should teach the client to choose music that matches their mood and preference.
Choice C reason: Practice using muscle relaxation techniques. This is the best instruction, as it can reduce the physical symptoms of anxiety. Muscle relaxation techniques involve tensing and relaxing different muscle groups in a systematic way, which can lower blood pressure, heart rate, and breathing rate. The nurse should teach the client how to perform muscle relaxation techniques and practice them regularly.
Choice D reason: Find outlets for more social interaction. This is not the best instruction, as it may not be feasible or helpful for all clients. Finding outlets for more social interaction may help some clients feel supported or connected, but it may also stress or overwhelm others. The nurse should teach the client to seek social support that is appropriate and comfortable for them.
Correct Answer is A
Explanation
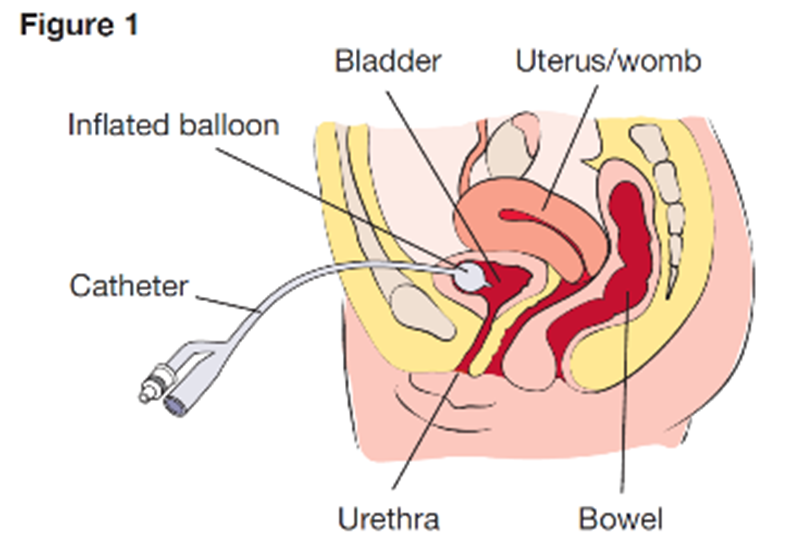
Choice A reason: Observing the insertion site of the suprapubic catheter is an essential assessment for the home health nurse, as this can help detect any signs of infection, inflammation, or leakage. Therefore, this is the correct choice.
Choice B reason: Palpating the flank area is not a necessary assessment for the home health nurse, as this is not related to the suprapubic catheter. This is a distractor choice.
Choice C reason: Measuring abdominal girth is not a relevant assessment for the home health nurse, as this is not affected by the suprapubic catheter. This is another distractor choice.
Choice D reason: Assessing the perineal area is not an important assessment for the home health nurse, as this is not involved in the suprapubic catheter. This is another distractor choice.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today