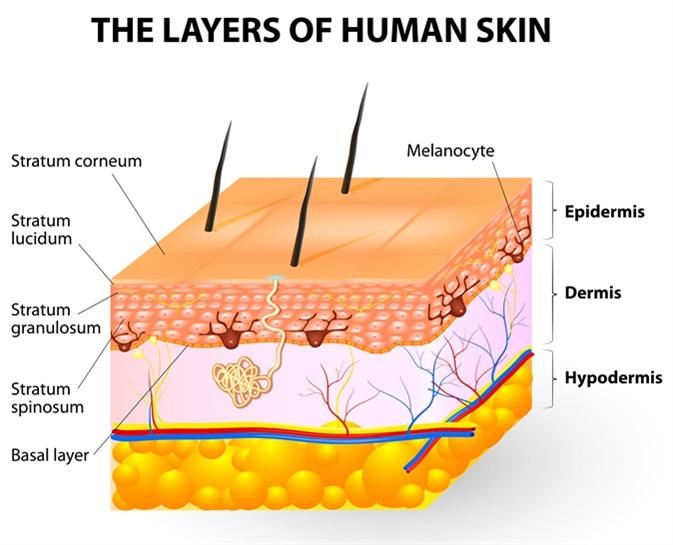
Melanocytes give rise to the pigment melanin, which is responsible for skin color. Where can the melanocytes be found?
Loose connective tissue
Epidermis
Dermis
Superficial fascia
The Correct Answer is B
A. Loose connective tissue:
Melanocytes are not typically found in loose connective tissue. Their primary location is within the epidermis, specifically in the basal layer, where they interact with keratinocytes to produce melanin and contribute to skin color. Loose connective tissue contains collagen and elastin fibers, as well as fibroblasts, but it does not house melanocytes.
B. Epidermis:
This is the correct answer. Melanocytes are primarily located in the basal layer of the epidermis, which is the deepest layer of the epidermis. These cells produce melanin, a pigment that helps protect the skin from UV radiation and determines skin color. Melanocytes are interspersed among keratinocytes in the epidermis and transfer melanin to keratinocytes to provide skin pigmentation.
C. Dermis:
The dermis is the layer of skin beneath the epidermis and consists of connective tissue, blood vessels, nerves, hair follicles, and sweat glands. While the dermis plays a crucial role in supporting and nourishing the epidermis, melanocytes are not primarily located in the dermis. They are confined to the basal layer of the epidermis.
D. Superficial fascia:
The superficial fascia, also known as the subcutaneous tissue or hypodermis, lies beneath the dermis and consists of adipose (fat) tissue and connective tissue. It provides insulation, energy storage, and cushioning for underlying structures. However, melanocytes are not typically found in the superficial fascia. They are restricted to the epidermis, specifically the basal layer, where they carry out their function of melanin production.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["E"]
Explanation
A. Increased pulse rate:
This is a common manifestation of fluid overload. Excess fluid volume can lead to an increase in cardiac output, causing the heart to pump faster and resulting in an increased pulse rate.
B. Decreased blood pressure:
Fluid overload typically leads to increased blood volume, which can initially cause an increase in blood pressure. However, as fluid overload progresses, it can lead to fluid redistribution, venous congestion, and decreased systemic vascular resistance, ultimately resulting in decreased blood pressure.
C. Skeletal muscle weakness:
Skeletal muscle weakness is not a direct manifestation of fluid overload. It is more commonly associated with electrolyte imbalances, such as hypokalemia or hypomagnesemia, which can occur as a consequence of fluid shifts but are not specific to fluid overload itself.
D. Warm and pink skin:
Warm and pink skin is not typically associated with fluid overload. Instead, it is more indicative of adequate tissue perfusion and oxygenation. In fluid overload, skin changes may include edema, cool and clammy skin due to venous congestion, or signs of skin breakdown in areas of pressure.
E. Distended neck veins:
Distended neck veins, specifically jugular venous distention (JVD), are commonly seen in patients with fluid overload, especially if there is right-sided heart failure or increased central venous pressure. JVD is a result of increased venous return to the heart due to fluid accumulation.
Correct Answer is ["B","D"]
Explanation
A. Cool the burn with ice water:
Not recommended: Cooling a burn with ice water directly is not recommended as it can lead to further tissue damage and complications. Instead, the burn should be cooled with cool (not cold) running water for a limited time and then covered with a clean, dry cloth.
B. Administer opioid analgesics:
Recommended: Severe burns can cause excruciating pain, and opioid analgesics are often necessary to manage this pain effectively. However, the specific opioid, dosage, and route of administration should be determined by the healthcare provider based on the client's condition and pain level.
C. Administer systemic antibiotics:
Not routinely recommended: Unless there are signs of infection or the burn involves deep tissue damage, systemic antibiotics are not typically administered prophylactically for burn injuries. However, if there are signs of infection, such as redness, swelling, warmth, or drainage from the burn site, antibiotic therapy may be initiated based on culture and sensitivity results.
D. Administer benzodiazepines for anxiety management:
Considered: Severe burns can cause significant psychological distress and anxiety in patients. Benzodiazepines may be considered to manage acute anxiety and agitation in these situations. However, the decision to administer benzodiazepines should be made based on the client's overall condition, vital signs, and response to non-pharmacological interventions for anxiety.
E. Lay the head of the bed flat:
Not recommended: In a client with severe burns who is experiencing increased work of breathing, anxiety, and rapid breathing, it is generally more beneficial to elevate the head of the bed slightly (semi-Fowler's position) to improve respiratory mechanics and reduce anxiety-related respiratory distress.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today