In caring for a client who requires seizure precautions, the practical nurse (PN) should ensure the ready availability of equipment to perform which procedure?
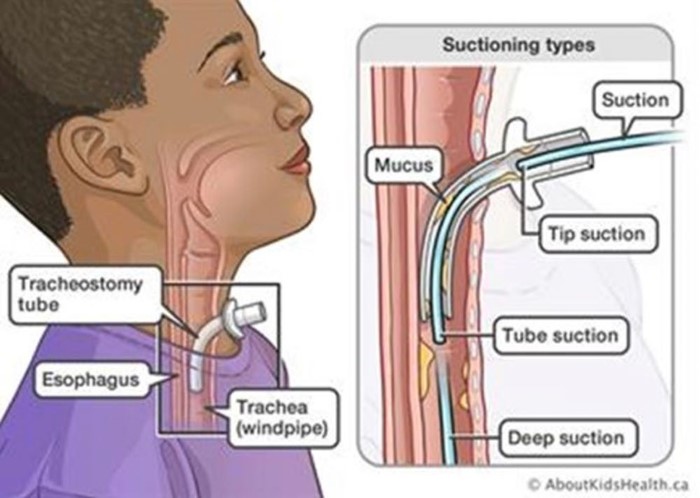
Suction the trachea.
Insert a urinary catheter.
Apply soft restraints.
Insert a nasogastric tube.
The Correct Answer is A
- Seizure precautions are measures taken to protect a client who is at risk of having a seizure, which is a sudden and abnormal electrical activity in the brain that can cause changes in behavior, movement, sensation, or consciousness. Seizure precautions include providing a safe environment, monitoring the client's vital signs and neurological status, administering anticonvulsant medications, and documenting the onset, duration, and characteristics of any seizure activity.
- One of the potential complications of a seizure is aspiration, which is the inhalation of foreign material into the lungs, such as saliva, vomit, or food. Aspiration can cause choking, pneumonia, or respiratory distress. To prevent or treat aspiration, the practical nurse (PN) should ensure the ready availability of equipment to perform suctioning of the trachea, which is the tube that connects the mouth and nose to the lungs. Suctioning of the trachea involves inserting a catheter through the nose or mouth into the trachea and applying negative pressure to remove any secretions or debris from the airway.
- Therefore, option A is the correct answer, while options B, C, and D are incorrect.
Option B is incorrect because inserting a urinary catheter is not related to seizure precautions or aspiration prevention.
Option C is incorrect because applying soft restraints may not be necessary or appropriate for a client who requires seizure precautions, as they may interfere with the natural movements of the seizure or cause injury to the client.
Option D is incorrect because inserting a nasogastric tube is not related to seizure precautions or aspiration prevention.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Hypoxemia is a condition of low oxygen levels in the blood. PEEP can actually improve oxygenation by preventing alveolar collapse and increasing functional residual capacity.
B. Tension pneumothorax is a life-threatening condition of air accumulation in the pleural space that causes increased intrathoracic pressure and compresses the lungs, heart, and great vessels. PEEP can increase the risk of tension pneumothorax by creating excessive positive pressure in the airways and alveoli.
C. Malignant hypertension is a severe form of high blood pressure that can cause organ damage and stroke. PEEP can cause a transient increase in blood pressure due to increased intrathoracic pressure, but it does not cause malignant hypertension.
D. Atelectasis is a condition of partial or complete lung collapse due to alveolar collapse or obstruction. PEEP can prevent or treat atelectasis by maintaining positive pressure in the airways and alveoli.
Correct Answer is C
Explanation
Choice A option:
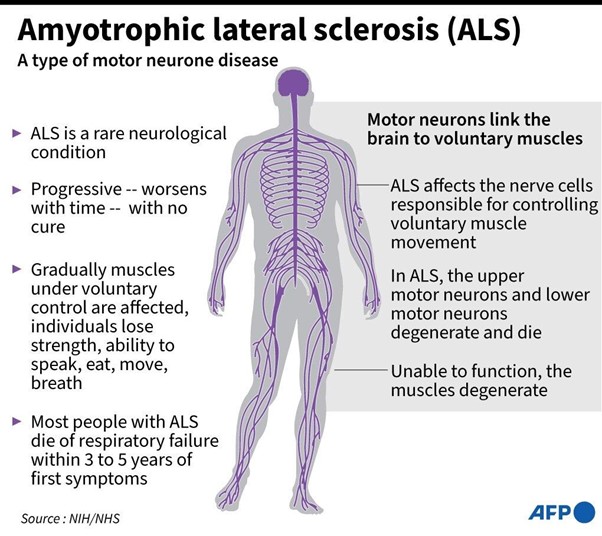
Dietitian should not be consulted: The dietitian is an essential team member and will work closely with the client to ensure proper nutrition and dietary management. However, in the context of dysphagia, the speech-language pathologist's expertise is needed to determine safe swallowing strategies and food modifications.
Choice B option:
Physical therapist should not be consulted: The physical therapist focuses on maintaining and improving the client's physical function and mobility. While important in ALS management, the physical therapist's role is not directly related to the immediate issue of dysphagia.
Choice C option:
The speech-language pathologist is the correct answer because it specializes in assessing and treating communication and swallowing disorders. In this case, the speech-language pathologist is essential in evaluating the client's swallowing function, recommending appropriate dietary modifications (texture and consistency of foods), and implementing swallowing exercises or strategies to improve swallowing safety.
Choice D option:
Occupational therapist should not be consulted: The occupational therapist assists clients in regaining or maintaining independence in daily living activities. While the occupational therapist may address some aspects of mealtime activities and adaptive strategies, the speech-language pathologist is more specialized in evaluating and treating swallowing difficulties in clients with ALS.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today