A nurse is providing dietary teaching for a client who has chronic obstructive pulmonary disease. Which of the following instructions should the nurse include?
"Use a bronchodilator 1 hour before eating."
"Eat 3 large meals each day."
"Limit water intake with meals."
"Reduce protein intake."
None
None
The Correct Answer is C
A. Administration of a prescribed bronchodilator is typically recommended approximately 30 minutes prior to meals rather than 1 hour. This pharmacological timing helps reduce dyspnea and facilitates easier deglutition and mastication by improving airflow. Using it too early may result in the peak therapeutic effect tapering off before the client finishes the meal.
B. Consuming 3 large meals each day is contraindicated for clients with chronic obstructive pulmonary disease because a distended stomach can exert upward pressure on the diaphragm. This abdominal crowding significantly increases the work of breathing and leads to early satiety or respiratory distress. Clients are instead encouraged to eat 5 to 6 small, frequent, nutrient-dense meals.
C. The nurse should instruct the client to limit water or fluid intake during the actual mealtime to prevent premature gastric distention. Early fullness from fluids reduces the client’s ability to consume essential solid nutrients and calories required to support the increased metabolic demands of labored breathing. Fluids should be consumed between meals to maintain adequate hydration and thin secretions.
D. Reducing protein intake is inappropriate because these clients require high-protein and high-calorie diets to prevent muscle wasting and support the respiratory muscles. The metabolic cost of breathing in chronic obstructive pulmonary disease is significantly elevated, often leading to a state of malnutrition or cachexia. Protein is vital for tissue repair and maintaining the functional integrity of the diaphragm.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","C","E"]
Explanation
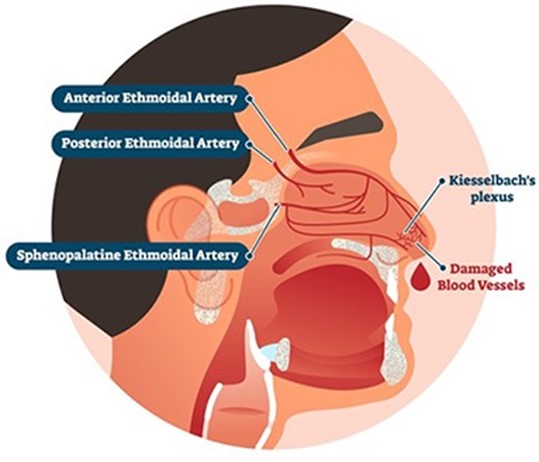
These actions help to control bleeding, reduce blood pressure, and promote clotting.
a. Tilt the client's head backward. This is not recommended, as it can cause blood to drain into the throat and increase the risk of aspiration, nausea, or vomiting.
d. Instruct the client to blow his nose. This is not advisable, as it can dislodge any clots that have formed and worsen bleeding.
Correct Answer is D
Explanation
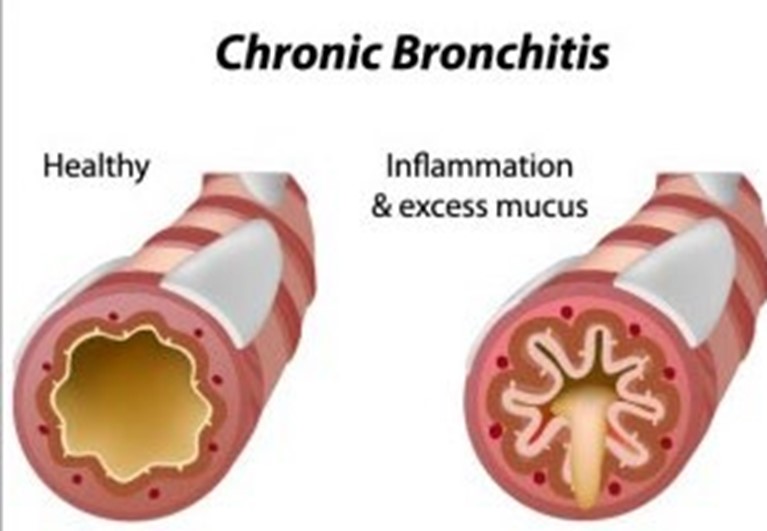
Smoking cessation is the most effective way to prevent chronic bronchitis, which is a type of chronic obstructive pulmonary disease (COPD) characterized by inflammation and excess mucus production in the
bronchi. Smoking is the main cause of chronic bronchitis, as it damages the cilia and mucous membranes of the airways, leading to chronic cough, sputum, and infection. Quitting smoking can reduce the risk of developing or worsening chronic bronchitis and improve lung function and quality of life.
a) Regular moderate exercise is beneficial for preventing chronic bronchitis, but not as effective as smoking cessation. Exercise can improve cardiovascular and respiratory health, increase oxygen delivery to the tissues, and enhance immune function. However, exercise alone cannot reverse the damage caused by smoking or prevent further deterioration of the airways.
b) Maintenance of ideal weight is beneficial for preventing chronic bronchitis, but not as effective as smoking cessation. Maintaining a healthy weight can reduce the workload on the heart and lungs, prevent obesity-related complications, and improve self-esteem and well-being. However, weight management alone cannot restore the normal structure and function of the airways or prevent chronic inflammation and mucus production.
c) Annual influenza immunization is beneficial for preventing chronic bronchitis, but not as effective as smoking cessation. Influenza immunization can protect against viral infections that can trigger or exacerbate chronic bronchitis symptoms, such as fever, cough, wheezes, and dyspnea. However, influenza immunization cannot prevent other causes of chronic bronchitis, such as bacterial infections, environmental pollutants, or genetic factors.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today