A nurse is preparing a client for a pelvic examination. Which of the following actions should the nurse take?
Assist the client to a prone position.
Ask the client to empty their bladder.
Instruct the client to douche.
Place the client’s arms over their head.
The Correct Answer is B
Ask the client to empty their bladder.
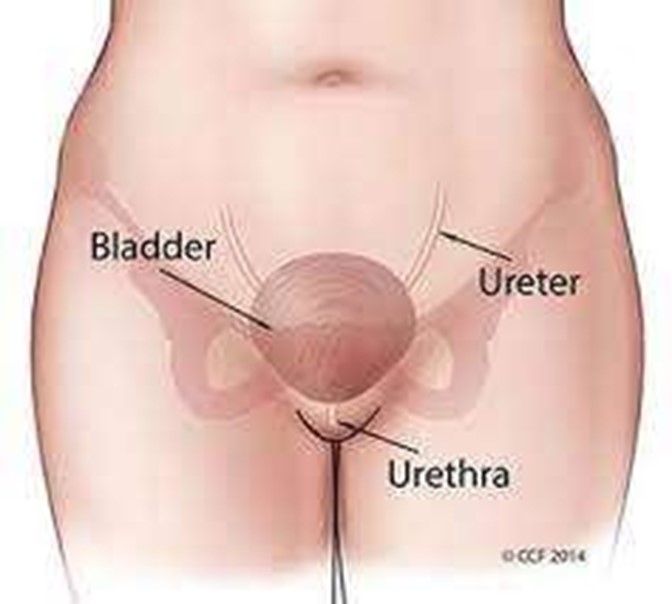
This is because a full bladder can interfere with the pelvic examination and cause discomfort to the client. The nurse should also instruct the client to avoid douching, using tampons, vaginal medications, sprays, powders, birth control foam, cream, or jelly for at least 24 hours before the exam.
Choice A is wrong because the client should be placed in a lithotomy position, not a prone position, for a pelvic examination.
Choice C is wrong because douching can alter the normal vaginal flora and pH, and increase the risk of infection.
Choice D is wrong because placing the client’s arms over their head can tighten the abdominal muscles and make the examination more difficult. The nurse should ask the client to place their arms at their sides or across their chest.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
“I will not play soccer until my doctor tells me I can.” This statement indicates that the client understands the risk of splenic rupture due to splenomegaly and the need to avoid contact sports until the spleen returns to normal size.
Choice A is wrong because antibiotics are not effective for infectious mononucleosis, which is caused by a virus.
Choice C is wrong because varicella booster is not related to infectious mononucleosis and there is no evidence that the client needs it.
Choice D is wrong because jaundice (yellowing of the eyes and skin) is not a common manifestation of infectious mononucleosis and may indicate another condition such as hepatitis.
Normal ranges for spleen size are 7 to 14 cm in length and 3 to 4 cm in thickness.
Correct Answer is C
Explanation
Blood glucose 130 mg/dL.
This is because the normal range of blood glucose for pregnant women is 70 - 110 mg/dL .
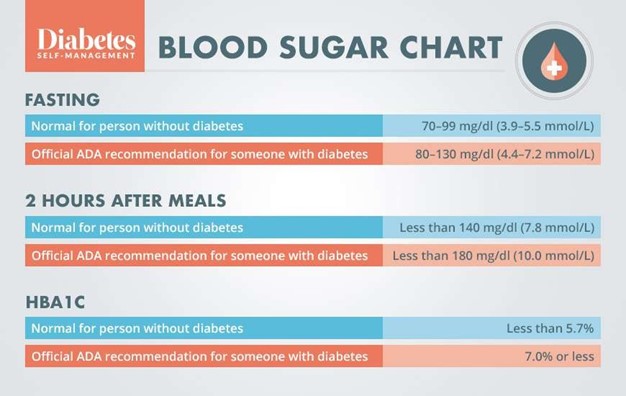
A blood glucose level of 130 mg/dL indicates gestational diabetes, which can have adverse effects on the mother and the fetus.
The nurse should report this finding to the provider and initiate interventions such as dietary counseling, glucose monitoring, and insulin therapy if needed.
Choice A is wrong because WBC 7,000/mm³ is within the normal range for pregnant women, which is 4,500 to 10,000 cells/mcL .
A low WBC count would indicate an increased risk of infection, while a high WBC count would indicate inflammation or infection.
Choice B is wrong because hemoglobin 13 g/dL is within the normal range for pregnant women, which is 11 to 14 g/dL .
A low hemoglobin level would indicate anemia, while a high hemoglobin level would indicate dehydration or polycythemia.
Choice D is wrong because RBC 5.8 million/mm³ is within the normal range for pregnant women, which is 4.2 to 5.9 million/mm³ .
A low RBC count would indicate anemia or hemorrhage, while a high RBC count would indicate dehydration or polycythemia.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today