A nurse is planning eating strategies with a client who has nausea from equilibrium imbalance. Which of the following strategies should the nurse recommend?
Serve hot foods at mealtime.
Provide low-fat carbohydrates with meals.
Encourage the client to eat even if nauseated.
Limit fluid intake between meals.
The Correct Answer is B
Choice B reason: Providing low-fat carbohydrates with meals can help reduce nausea and vomiting in clients who have equilibrium imbalance. Low-fat carbohydrates are easy to digest and can provide energy and prevent hypoglycemia. Examples of low-fat carbohydrates are crackers, toast, rice, and noodles.
Choice A reason: Serving hot foods at mealtime is not a good strategy for clients who have nausea from equilibrium imbalance. Hot foods can have strong odors and flavors that can trigger nausea and vomiting. Cold or room-temperature foods are more tolerable and less stimulating for the senses.
Choice C reason: Encouraging the client to eat even if nauseated is not a helpful strategy for clients who have nausea from equilibrium imbalance. Forcing the client to eat can worsen nausea and vomiting and cause discomfort and distress. The nurse should respect the client's preferences and appetite and offer small, frequent meals and snacks.
Choice D reason: Limiting fluid intake between meals is not a necessary strategy for clients who have nausea from equilibrium imbalance. Fluid intake is important to prevent dehydration and electrolyte imbalance, which can occur due to vomiting. The nurse should encourage the client to drink fluids between meals, but avoid drinking fluids with meals, as this can cause bloating and fullness.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
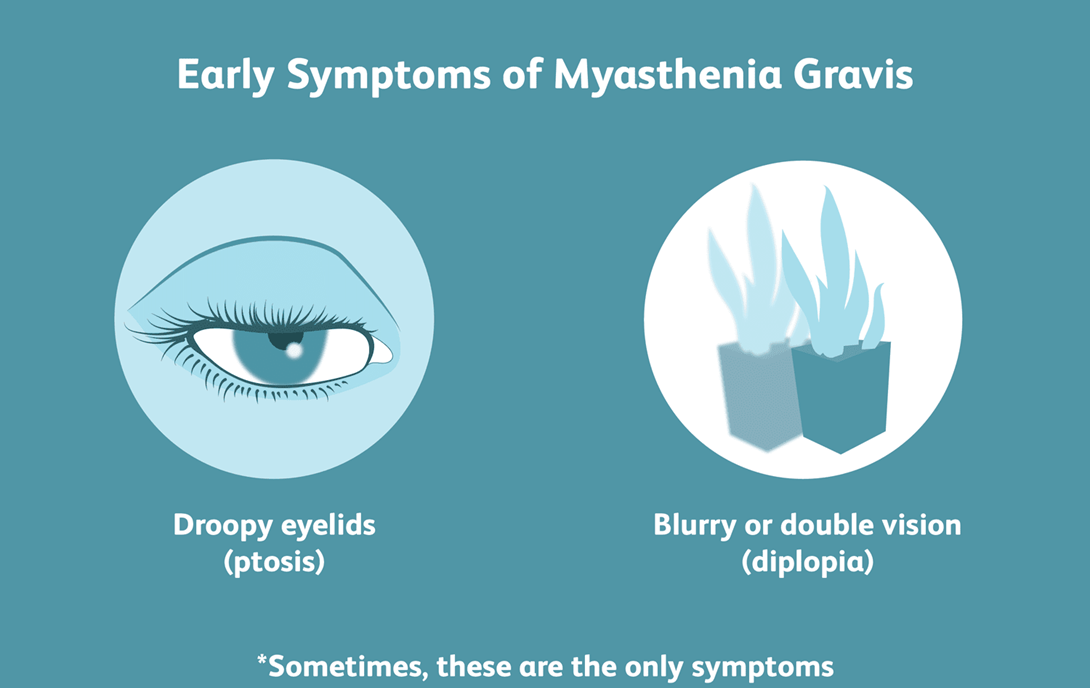
Choice A reason: Anticholinesterase medications should be taken 30 minutes before meals, not with meals. This is because they enhance the action of acetylcholine, which improves muscle strength and swallowing ability.
Choice B reason: Positioning the head of the client's bed to 40° while eating helps prevent aspiration and facilitates swallowing. This is the best action for the nurse to take for a client who has myasthenia gravis.
Choice C reason: Encouraging the client to lie down after eating is not advisable, as it increases the risk of aspiration and reflux. The client should remain upright for at least 30 minutes after eating.
Choice D reason: Providing the client with food cut into small bites is not enough to ensure safe and adequate nutrition. The client may still have difficulty swallowing and chewing. The nurse should also offer soft, moist, and easy-to-swallow foods, and avoid foods that are dry, sticky, or hard.
Correct Answer is B
Explanation
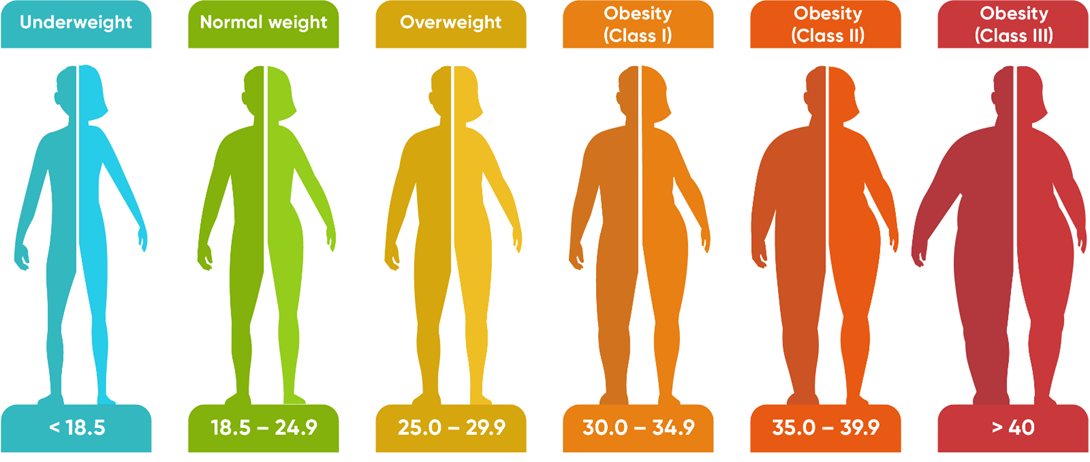
Choice A reas on: Weight gain of 0.45 kg (1 lb) per week is not within the expected reference range for a client who is in the second trimester of pregnancy and has a normal BMI. The recommended weight gain for this client is 0.35 to 0.5 kg (0.8 to 1 lb) per week.
Choice B reason: Intake of 200 extra calories per day is within the expected reference range for a client who is in the second trimester of pregnancy and has a normal BMI. The recommended caloric intake for this client is 2200 to 2900 calories per day, which is about 340 to 450 calories more than the pre-pregnancy intake.
Choice C reason: Intake of 100 extra calories per day is not within the expected reference range for a client who is in the second trimester of pregnancy and has a normal BMI. The recommended caloric intake for this client is 2200 to 2900 calories per day, which is about 340 to 450 calories more than the pre-pregnancy intake.
Choice D reason: Weight gain of 0.91 kg (2 lb) per week is not within the expected reference range for a client who is in the second trimester of pregnancy and has a normal BMI. The recommended weight gain for this client is 0.35 to 0.5 kg (0.8 to 1 lb) per week.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today