A nurse is planning care for a client who has a history of seizures. Which of the following interventions should the nurse include in the plan of care?
Plan to insert an oral airway if seizure activity begins.
Plan to administer pain medication after the seizure.
Pad the side rails of the client's bed with blankets.
Place the client in a supine position during a seizure.
The Correct Answer is C
Choice A rationale:
Planning to insert an oral airway if seizure activity begins is not a suitable intervention for a client with a history of seizures. During a seizure, it's essential to protect the client from injury by preventing them from aspirating secretions or foreign objects. However, inserting an oral airway during an active seizure can be dangerous and lead to injury.
Choice B rationale:
Administering pain medication after the seizure is not a priority intervention. While some clients may experience muscle soreness or discomfort following a seizure, the primary focus during and immediately after a seizure is ensuring the client's safety and preventing injury. Pain medication can be considered later if necessary.
Choice C rationale:
The correct choice is to pad the side rails of the client's bed with blankets. This intervention aims to prevent injury if the client experiences a seizure and comes into contact with the bed rails. Padding the side rails can reduce the risk of trauma and minimize the potential for harm during a seizure episode.
Choice D rationale:
Placing the client in a supine position during a seizure is not recommended. It's important to position the client on their side (lateral recumbent position) during a seizure to allow any oral secretions or vomit to drain from the mouth, reducing the risk of aspiration. Placing the client supine could obstruct the airway and increase the risk of aspiration.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale:
Determining what the client knows about coronary artery disease is an important step in assessing the client's baseline knowledge. However, it's not the first step in developing teaching strategies. First, the nurse should establish a collaborative relationship with the client to set mutual learning goals.
Choice B rationale:
Identifying resources that will help support the client's lifestyle changes is an essential aspect of the teaching process, but it's not the initial step. The nurse needs to work with the client to set goals and develop a plan before seeking external resources.
Choice C rationale:
Establishing mutual learning goals with the client is the most crucial first step. This approach ensures that the teaching plan aligns with the client's needs and preferences, fostering a sense of partnership and increasing the likelihood of successful lifestyle changes.
Choice D rationale:
Scheduling a teaching session about coronary artery disease in a quiet setting is an important consideration for effective teaching, but it comes after the nurse and the client have identified mutual learning goals. The nurse should engage the client in goal-setting before planning specific teaching sessions.
Correct Answer is B
Explanation
Choice A rationale:
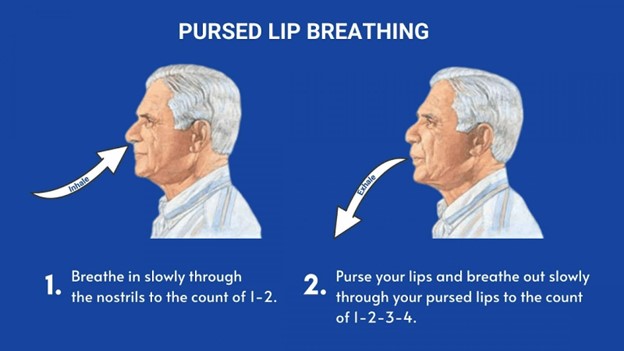
Lying down while practicing pursed-lip breathing is not the correct instruction. Pursed-lip breathing is usually performed in a sitting or standing position. Lying down can restrict lung expansion and may not effectively support the purpose of this breathing technique, which is to improve airway pressure and reduce air trapping.
Choice B rationale:
"Exhale slowly through your mouth" is the correct instruction for pursed-lip breathing. This technique involves inhaling through the nose for a count of two and exhaling slowly and steadily through pursed lips for a count of four. The goal is to promote better exhalation, prevent airway collapse, and improve oxygen exchange. The rationale behind this choice is grounded in the mechanics of pursed-lip breathing, which helps create backpressure in the airways, maintaining them open and aiding in proper exhalation.
Choice C rationale:
Inhaling through pursed lips contradicts the proper sequence of pursed-lip breathing. The technique involves inhaling through the nose and exhaling through pursed lips. Inhaling through pursed lips would not provide the intended benefits of the technique.
Choice D rationale:
"Puff your cheeks when exhaling" is not the correct instruction. Puffing the cheeks during exhalation does not contribute to the effectiveness of pursed-lip breathing. This action could potentially impede proper exhalation and defeat the purpose of the technique, which is to control airflow and improve breathing efficiency.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today