A nurse is performing a neurological assessment for a client who has head trauma. Which of the following assessments will give the nurse information about the function of cranial nerve III?
Ask the client to shrug his shoulders against passive resistance
Instruct the client to look up and down without moving his head
Observe the client's ability to smile and frown
Have the client stand with his eyes closed and touch his nose
The Correct Answer is B
Choice A: Ask the client to shrug his shoulders against passive resistance is not an assessment that will give the nurse information about the function of cranial nerve III. This assessment will test the function of cranial nerve XI, which is the accessory nerve. The accessory nerve innervates the trapezius and sternocleidomastoid muscles, which are involved in shoulder and neck movements.
Choice B: Instruct the client to look up and down without moving his head is an assessment that will give the nurse information about the function of cranial nerve III. Cranial nerve III is the oculomotor nerve, which innervates four of the six extraocular muscles that control eye movements. The oculomotor nerve also controls pupil size and lens shape. By instructing the client to look up and down without moving his head, the nurse can assess the ability of the oculomotor nerve to move the eyes vertically and adjust to different distances.
Choice C: Observe the client's ability to smile and frown is not an assessment that will give the nurse information about the function of cranial nerve III. This assessment will test the function of cranial nerve VII, which is the facial nerve. The facial nerve innervates the muscles of facial expression, which are involved in smiling, frowning, blinking, and other facial movements.
Choice D: Have the client stand with his eyes closed and touch his nose is not an assessment that will give the nurse information about the function of cranial nerve III. This assessment will test the function of cranial nerve VIII, which is the vestibulocochlear nerve. The vestibulocochlear nerve innervates the inner ear and is responsible for hearing and balance. By having the client stand with his eyes closed and touch his nose, the nurse can assess the ability of the vestibulocochlear nerve to maintain equilibrium and coordination.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
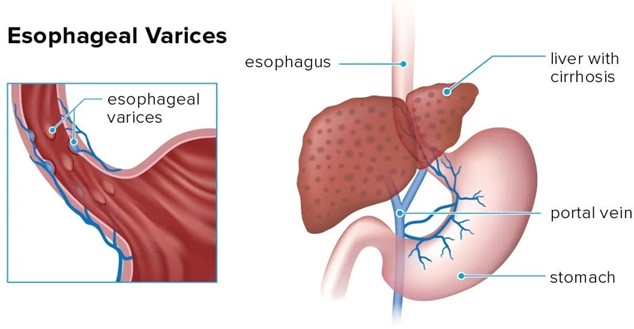
Choice A: Provide frequent oral and nares care is the correct action for the nurse to take. Oral and nares care can help prevent infection, dryness, and irritation of the mucous membranes, which can be damaged by the pressure and friction of the tube. The nurse should also monitor the tube position, secure it with tape, and keep scissors at the bedside in case of emergency deflation.
Choice B: Keep the client in a supine position is not the correct action for the nurse to take. The supine position can increase the risk of aspiration, regurgitation, and gastric distension, which can worsen the bleeding and compromise the airway. The nurse should elevate the head of the bed to at least 30 degrees and use a semi-Fowler's or high-Fowler's position.
Choice C: Ambulating the client four times per day is not the correct action for the nurse to take. Ambulation can increase abdominal pressure and dislodge the tube, which can cause bleeding and perforation. The nurse should keep the client on bed rest and use passive range-of-motion exercises to prevent complications such as thromboembolism and muscle atrophy.
Choice D: Encouraging the client to consume clear liquids is not the correct action for the nurse to take. Clear liquids can increase gastric volume and acidity, which can aggravate the bleeding and interfere with hemostasis. The nurse should maintain a nothing-by-mouth status and provide intravenous fluids and nutrition as prescribed.
Correct Answer is D
Explanation
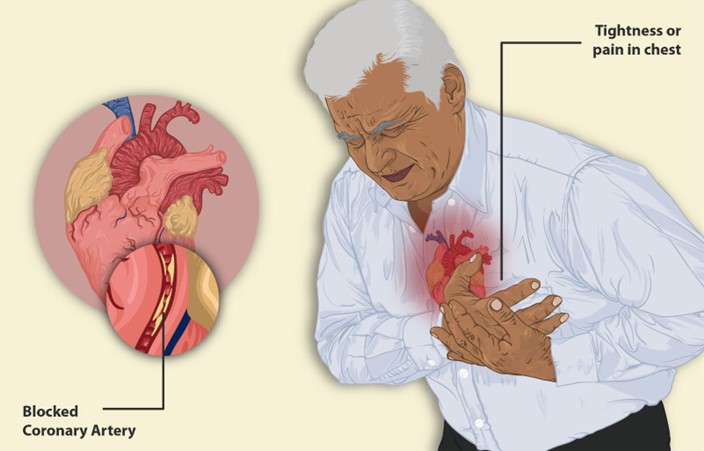
Choice A Reason: This is incorrect. Anginal pain usually lasts less than 20 min and subsides with rest or medication. Pain that lasts longer than 20 min may indicate a myocardial infarction.
Choice B Reason: This is incorrect. Anginal pain usually responds to rest and organic nitrates, such as nitroglycerin. Pain that does not improve with these measures may indicate unstable angina or a myocardial infarction.
Choice C Reason: This is incorrect. Anginal pain is not affected by the position of the client. Pain that is relieved by sitting up may indicate pericarditis or pleurisy.
Choice D Reason: This is correct. Anginal pain is caused by a temporary imbalance between the oxygen demand and supply of the myocardium. Factors that increase the oxygen demand, such as exertion, anxiety, cold, or heavy meals, can trigger anginal pain.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today