A nurse is contributing to the plan of care for a client who has Parkinson's disease. Which of the following interventions should the nurse plan to include?
Restrict the client's fluid intake
Keep suction equipment at the client's bedside
Instruct the client to look down when ambulating
Position the client supine after eating
The Correct Answer is B
b. Keep suction equipment at the client's bedside.
The nurse should plan to include keeping suction equipment at the client's bedside as an intervention for a client with Parkinson's disease. Parkinson's disease can cause dysphagia (difficulty swallowing) and an increased risk of aspiration. Having suction equipment readily available allows for prompt intervention in case of choking or aspiration episodes, ensuring the client's safety.
Explanation for the other options:
a. Restrict the client's fluid intake: Restricting the client's fluid intake is not typically indicated in the care of a client with Parkinson's disease. Adequate hydration is important for overall health and well-being. However, specific fluid restrictions may be necessary in certain situations, such as if the client has coexisting conditions like heart failure or kidney disease, which should be assessed and determined by the healthcare provider.
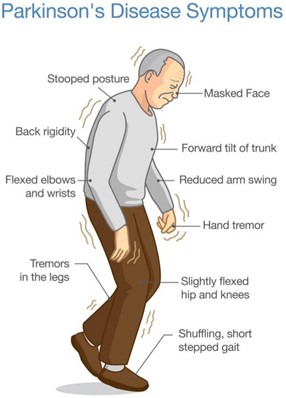
c. Instruct the client to look down when ambulating: In Parkinson's disease, individuals often experience a forward-flexed posture and a shuffling gait. Instructing the client to look down when ambulating is not an appropriate intervention. Instead, the nurse should encourage the client to maintain an upright posture, take smaller steps, and focus on taking deliberate and controlled movements to promote stability and reduce the risk of falls.
d. Position the client supine after eating: Positioning the client supine after eating is not recommended for a client with Parkinson's disease. This position can increase the risk of aspiration, as it may promote reflux and regurgitation of stomach contents. Instead, the nurse should advise the client to maintain an upright position, such as sitting in a chair or using a recliner with appropriate head support, to aid digestion and reduce the risk of aspiration.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
The nurse should administer scheduled pain medications to a client who is near death. This is an important nursing intervention to ensure that the client is comfortable and free from pain.
b) Providing oral care every 6 hours is important, but it may not be the highest priority for a client who is near death.
c) Administering liquids using a syringe may not be necessary or appropriate for a client who is near death.
d) Whispering when talking to family members is not necessary. The nurse should communicate openly and honestly with the family members.
Correct Answer is ["B"]
Explanation
Answer: B
Rationale:
A) Use written signs to assist the client with locating the bathroom: While written signs may be helpful in the earlier stages of Alzheimer's disease, as the disease progresses, clients may lose the ability to read and comprehend written language. Visual cues, such as pictures or color-coded indicators, tend to be more effective in helping clients navigate their environment.
B) Limit the number of choices for the client: Limiting choices reduces confusion and anxiety for clients with Alzheimer's disease. Providing too many options can overwhelm them, making decision-making difficult. Offering simple, clear choices helps to maintain a sense of autonomy while minimizing stress.
C) Provide a stimulating environment for the client: Although some stimulation can be beneficial, excessive stimulation can overwhelm a client with Alzheimer's disease, leading to agitation and confusion. It's important to create a calm, structured environment that promotes safety and reduces anxiety.
D) Use confrontation to manage the client’s behavior: Confrontation should be avoided when managing the behavior of clients with Alzheimer's disease. Confronting or challenging them can increase agitation and lead to further confusion. Instead, caregivers should use distraction, redirection, and a calm approach to manage difficult behaviors effectively.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today