A nurse is caring for a client who is scheduled for surgery.
Exhibit 1
Medical History
0800:
Client has a history of malnutrition, hyperlipidemia, and diabetes mellitus.
Mini Nutritional Assessment screening tool score of 7 points (0 to 14 points)
The nurse is reviewing the client's medical record. Which of the following findings places the client at risk for delayed wound healing? Select all that apply
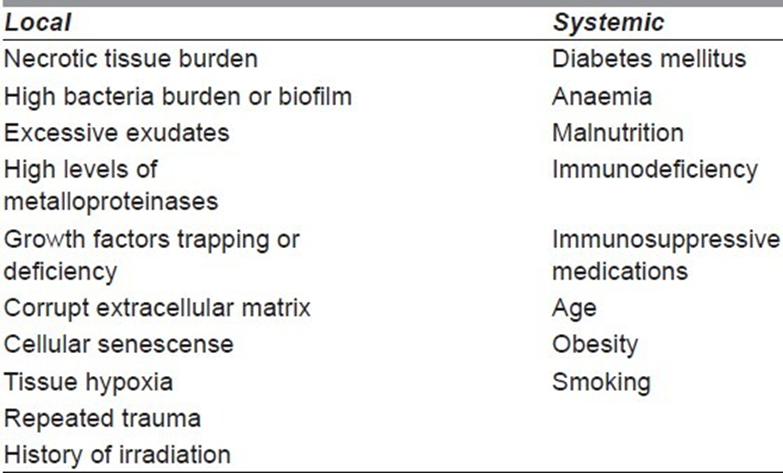
History of diabetes mellitus
Cholesterol level
Prealbumin level
History of hyperlipidemia
Mini Nutritional Assessment screening tool score
History of malnutrition
Correct Answer : A,C,E,F
A. History of diabetes mellitus: This is correct. Diabetes mellitus can lead to delayed wound healing due to various factors, including impaired circulation, neuropathy, and compromised immune function.
B. Cholesterol level: While abnormal cholesterol levels can impact cardiovascular health, they are not directly linked to delayed wound healing unless they are part of a broader metabolic disorder or condition that affects vascular health.
C. Prealbumin level: Prealbumin is a marker of nutritional status. Low prealbumin levels can indicate malnutrition, which is a risk factor for delayed wound healing.
D. History of hyperlipidemia: Hyperlipidemia refers to high levels of fats (lipids) in the blood, such as cholesterol and triglycerides. While hyperlipidemia is associated with cardiovascular risk, it is not a direct risk factor for delayed wound healing unless it is part of a broader metabolic syndrome or condition affecting vascular health.
E. Mini Nutritional Assessment screening tool score: This is correct. The Mini Nutritional Assessment (MNA) screening tool assesses nutritional status, and a low score indicates malnutrition or nutritional deficiencies, which can contribute to delayed wound healing.
F. History of malnutrition: This is correct. Malnutrition, whether due to inadequate intake, absorption issues, or other factors, is a significant risk factor for delayed wound healing as it affects the body's ability to repair tissues and fight infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
No explanation
Correct Answer is A
Explanation
A. Assault.
Assault is the threat or apprehension of harmful or offensive contact. In this scenario, the nurse is making a threat to administer medication by injection if the client doesn't comply with swallowing pills. Even though the nurse hasn't physically carried out the action yet, the threat itself constitutes assault. The client feels threatened by the nurse's statement, creating apprehension of harm or offensive contact.
B. Defamation: Defamation involves making false statements that harm a person's reputation. There is no indication of defamation in this scenario.
C. Battery: Battery involves the intentional and unauthorized touching of another person. While administering medication by injection without consent could be considered battery, the nurse has only made a threat at this point, not carried out the action.
D. Invasion of privacy: Invasion of privacy involves intruding into someone's private affairs without permission. There is no indication of invasion of privacy in this scenario.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today