A nurse is caring for a client who is 1 day postpartum and breastfeeding her newborn. The client reports sore nipples. Which of the following actions should the nurse take?
Instruct the client to wait 4 hours between daytime feedings.
Offer supplemental formula between the newborn's feedings.
Have the client limit the length of breastfeeding to 5 minutes per breast.
Assess the newborn's latch while breastfeeding.
Assess the newborn's latch while breastfeeding.
The Correct Answer is D
Sore nipples are a common problem for breastfeeding mothers, especially in the first few days or weeks after delivery. They can cause pain, discomfort, and frustration, and may interfere with breastfeeding success and satisfaction. The most common cause of sore nipples is poor latch, which means that the newborn does not attach to the breast correctly and does not suckle effectively. Poor latch can result from various factors, such as improper positioning, tongue-tie, inverted or flat nipples, engorgement, or thrush.
The nurse should assess the newborn's latch while breastfeeding to identify and correct any problems that may cause sore nipples. The nurse should observe the following signs of a good latch:
- The newborn's mouth is wide open and covers most of the areola (the dark area around the nipple).
- The newborn's chin and nose touch the breast, and the cheeks are rounded and not dimpled.
- The newborn's tongue is visible under the lower lip and curls around the breast.
- The newborn's lips are flanged outwards and not tucked inwards.
- The newborn's jaw moves rhythmically and smoothly, and swallowing sounds are audible.
- The mother feels a gentle tugging sensation on the nipple, but no pain or pinching.
The nurse should also teach the mother how to achieve a good latch by using different positions, supporting the breast with her hand, tickling the newborn's lower lip with her nipple, and bringing the newborn to the breast when their mouth is wide open. The nurse should also encourage the mother to seek help from a lactation consultant or a peer support group if she has persistent or severe nipple pain.
a) Instructing the client to wait 4 hours between daytime feedings is not an appropriate action for the nurse to take. This may reduce nipple soreness temporarily, but it can also cause breast engorgement, milk supply reduction, mastitis, or poor weight gain in the newborn. The nurse should advise the client to feed the newborn on demand, usually every 1.5 to 3 hours during the day and every 3 to 4 hours at night.
b) Offering supplemental formula between the newborn's feedings is not an appropriate action for the nurse to take. This may interfere with breastfeeding initiation and establishment, as it can reduce the mother's milk supply, confuse the newborn's sucking pattern, increase the risk of nipple preference or rejection, and expose the newborn to potential allergens or infections. The nurse should support exclusive breastfeeding for the first six months of life, unless there is a medical indication for supplementation.
c) Having the client limit the length of breastfeeding to 5 minutes per breast is not an appropriate action for the nurse to take. This may not be enough time for the newborn to get enough milk, especially the hindmilk that is richer in fat and calories. It may also prevent proper drainage of the breast and lead to engorgement or mastitis. The nurse should advise the client to let the newborn feed until they are satisfied and release the breast on their own, which may take 10 to 20 minutes per breast on average.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
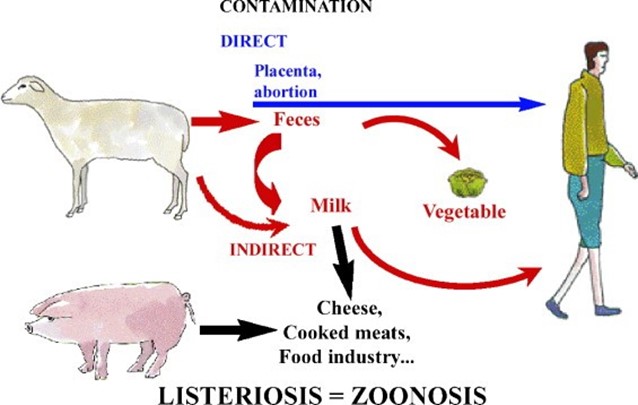
Listeriosis is a foodborne illness that can be very dangerous during pregnancy. It is caused by eating foods contaminated with the bacterium Listeria monocytogenes, which can grow well at refrigerator temperatures. Listeriosis can cause miscarriage, stillbirth, preterm labor, and serious illness or death in newborns. Pregnant women are 10 times more likely than other people to get Listeria infection¹.
To prevent listeriosis, pregnant women should avoid certain types of food that are more likely to be contaminated with Listeria, such as:
- Hot dogs and deli meats, unless they are reheated until steaming hot
- Soft cheeses made from unpasteurized milk, such as feta, brie, camembert, blue-veined cheeses, and
queso fresco
- Refrigerated pâtés or meat spreads
- Refrigerated smoked seafood, such as salmon, trout, whitefish, cod, tuna, or mackerel
- Raw or undercooked meat, poultry, seafood, or eggs
- Unpasteurized milk or dairy products
- Unwashed fruits and vegetables
Grilled chicken on a bun is a safe choice for lunchtime because the chicken is cooked and the bun is not likely to be contaminated with Listeria. However, the other options are not safe for pregnant women because they may contain Listeria or other harmful bacteria. A hot dog at the ballpark may not be reheated enough to kill Listeria. A seafood salad from the grocery store may contain refrigerated smoked seafood or mayonnaise made from raw eggs. Soft cheese is often made from unpasteurized milk and can harbor Listeria.
The other options are incorrect because they may expose the client to Listeria or other harmful bacteria, as I explained in my previous response. Let me summarize the reasons for you:
b) "I can still have a hot dog at the ballpark. This is incorrect because hot dogs and deli meats may contain Listeria unless they are reheated until steaming hot. A hot dog at the ballpark may not be hot enough to kill the bacteria.
c) "I can purchase a seafood salad from the grocery store." This is incorrect because seafood salad may contain refrigerated smoked seafood or mayonnaise made from raw eggs. Refrigerated smoked seafood can harbor Listeria and raw eggs can contain Salmonella or other bacteria that can cause food poisoning.
d) "I can have a mid-day snack with soft cheese.” This is incorrect because soft cheese made from unpasteurized milk can be contaminated with Listeria. Examples of soft cheese are feta, brie, camembert, blue-veined cheeses, and queso fresco.
Correct Answer is A
Explanation
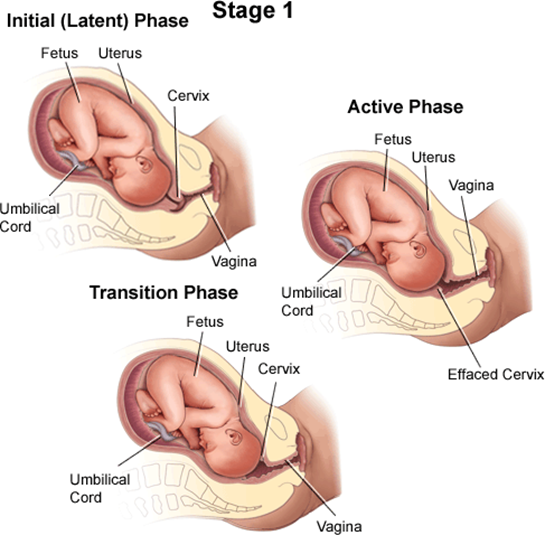
A client who is in labor and reports an urge to have a bowel movement during contractions may be experiencing the transition phase of labor, which is the last and most intense part of the first stage of labor¹². The transition phase occurs when the cervix dilates from 8 to 10 cm and the baby descends into the birth canal¹². The pressure of the baby's head on the rectum can cause a sensation of needing to defecate¹². The transition phase can last from 15 minutes to an hour or more, and it can be accompanied by other signs, such as strong, regular, and painful contractions lasting 60 to 90 seconds; increased bloody show; nausea and vomiting; shaking and shivering; and emotional changes such as irritability, anxiety, or excitement¹²³.
The nurse should reassess the client who reports an urge to have a bowel movement during contractions because this may indicate that the client is close to delivering the baby and needs to be prepared for the second stage of labor, which involves pushing and giving birth¹². The nurse should check the client's cervical dilation, fetal heart rate, and maternal vital signs, and notify the provider if the client is fully dilated or shows signs of fetal or maternal distress¹². The nurse should also support the client's coping strategies, such as breathing techniques, relaxation methods, or pain relief options, and encourage the client not to push until instructed by the provider¹².
b) A sense of excitement and warm, flushed skin are not signs that require reassessment by the nurse. These are normal emotional and physiological responses to labor that reflect increased adrenaline levels and blood flow¹⁴. They do not indicate any complications or imminent delivery.
c) Progressive sacral discomfort during contractions is not a sign that requires reassessment by the nurse. This is a common symptom of labor that results from the pressure of the baby's head on the sacrum and nerves in the lower back¹⁴. It does not indicate any problems or imminent delivery.
d) Intense contractions lasting 45 to 60 seconds are not signs that require reassessment by the nurse. These are typical characteristics of active labor contractions, which occur when the cervix dilates from 4 to 8 cm¹⁴. They do not indicate any complications or imminent delivery.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today