A nurse is assessing an older adult client. Which of the following findings should the nurse expect?
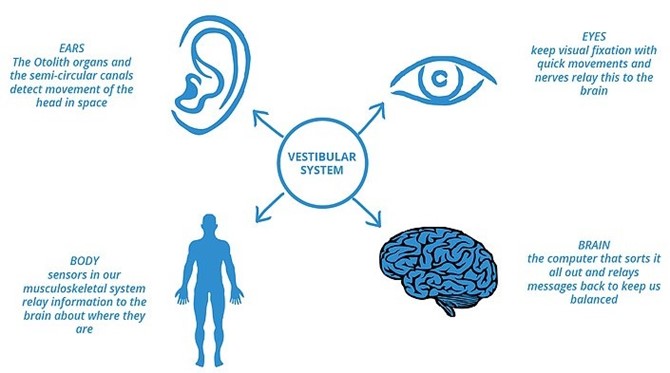
Decreased sense of balance
Nighttime urinary incontinence
Heightened sense of pain
Increased nighttime sleeping
The Correct Answer is A
As individuals age, it is common for them to experience a decreased sense of balance. This can be attributed to age-related changes in the musculoskeletal system, sensory perception, and coordination. The inner ear, which plays a vital role in maintaining balance, undergoes natural degenerative changes over time. Additionally, age-related decline in muscle strength and flexibility can contribute to difficulties in maintaining balance. Therefore, a nurse assessing an older adult client should expect a decreased sense of balance as a common finding.
- Nighttime urinary incontinence: While nighttime urinary incontinence can occur in some older adults, it is not a universal finding. It is important to avoid making assumptions or generalizations about older adults experiencing urinary incontinence. Each individual's urinary function can vary, and incontinence can be influenced by various factors such as overall health, bladder capacity, medication use, and underlying medical conditions.
- Heightened sense of pain: Older adults may experience changes in pain perception due to age-related physiological changes and medical conditions. However, it is not a predictable or expected finding for all older adult clients. Pain perception can vary among individuals based on their overall health, chronic conditions, and individual pain thresholds. Therefore, while some older adults may experience heightened pain sensitivity, it is not a universal expectation.
- Increased nighttime sleeping: Sleep patterns can change with age, and older adults may experience alterations in their sleep-wake cycles. However, increased nighttime sleeping is not a definitive finding that applies to all older adult clients. Sleep patterns can vary greatly among individuals, and some older adults may experience decreased sleep duration or disrupted sleep rather than increased nighttime sleeping.
In summary, the nurse should expect a decreased sense of balance as a common finding when assessing an older adult client. It is important to approach each individual as unique and recognize that other findings such as nighttime urinary incontinence, heightened sense of pain, or increased nighttime sleeping may or may not be present, as they can vary among older adults based on individual factors.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
The nurse should respect the client's autonomy and right to make decisions about their own care. Referring the client to hospice care is an appropriate response because it provides the client with support and care in their own home.
Options b, c, and d are not appropriate responses because they do not respect the client's autonomy.
Option b suggests that the client needs to discuss their decision with their family before making a decision, which may not be necessary or desired by the client.
Option c confronts the client with the reality of their illness in a potentially insensitive manner.
Option d suggests that the client is giving up too soon, which may not be an accurate or helpful assessment of the situation.
Correct Answer is C
Explanation
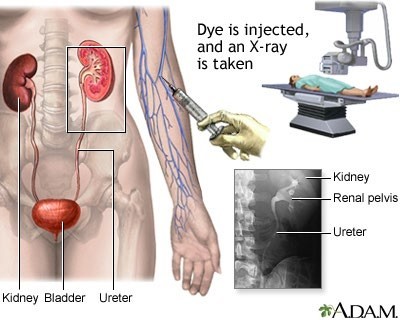
The nurse should assist the client with a bowel cleansing before an intravenous pyelogram. This helps to ensure that the bowel is empty and that the images obtained during the procedure are clear. The other
a. Oral contrast is not typically used for an intravenous pyelogram.
b. Pain in the suprapubic region is not a common side effect of an intravenous pyelogram.
d. Removing metal objects is important for procedures that use magnetic resonance imaging (MRI), but it is not necessary for an intravenous pyelogram.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today