A nurse identifies that a medication is ordered for the client as twice the regular dosage. What action should the nurse take?
Administer the medication as ordered.
Administer the standard dose and notify the prescriber.
Check to see if previous nurse gave the medication as ordered.
Collaborate with the prescriber regarding the ordered dose.
The Correct Answer is D
Collaborate with the prescriber about the order. This is because the nurse has a responsibility to ensure the safety and effectiveness of the medication administration and to question any orders that seem inappropriate or unclear. The nurse should not administer the medication as ordered without verifying it first, as this could cause harm to the client or result in a medication error. The nurse should not check to see if previous shift nurses gave the medication, as this does not address the issue of the current order and could lead to missed or duplicated doses. The nurse should not administer only the standard dose of the medication, as this could be against the prescriber’s intention and could compromise the client’s treatment or outcome.
Choice A is wrong because it does not follow the principle of safe medication administration and could put the client at risk of adverse effects or overdose.
Choice B is wrong because it does not respect the prescriber’s authority and could result in underdosing or ineffective therapy for the client.
Choice C is wrong because it does not solve the problem of the current order and could cause confusion or inconsistency in the medication administration.
Choice D is correct because it demonstrates critical thinking and professional accountability, and ensures that the order is appropriate and accurate for the client’s condition and needs.
The normal ranges for medication dosages depend on various factors, such as the type of medication, the route of administration, the client’s age, weight, renal function, liver function, and other comorbidities.
The nurse should always consult reliable sources of information, such as drug guides, pharmacists, or prescribers, to determine the safe and effective dosages for each client
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
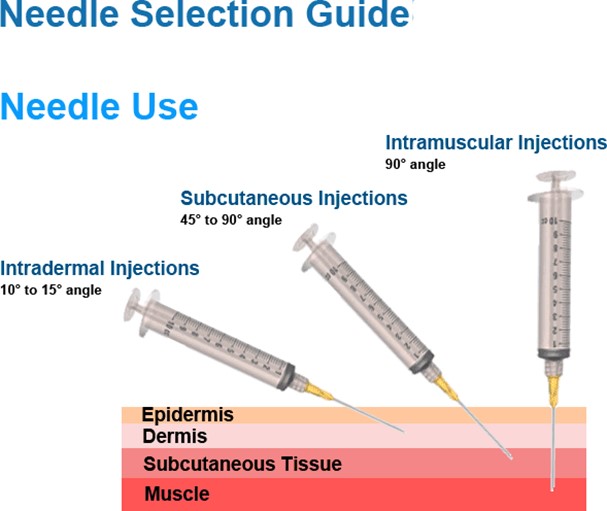
This needle size is appropriate for an intramuscular injection into the deltoid of a 175-pound adult male with a viscous fluid.
The needle length should be long enough to reach the muscle through the subcutaneous tissue, and the needle gauge should be suitable for the viscosity of the fluid. A 23-gauge needle is a common choice for intramuscular injections.
Choice A is wrong because a 1/2 inch needle is too short to reach the deltoid muscle in an adult male.
Choice C is wrong because a 1-1/2 inch needle is too long and may cause injury to the underlying nerves or blood vessels.
Choice D is wrong because a 16-gauge needle is too large and may cause excessive tissue trauma and pain.
Correct Answer is D
Explanation
What are the client’s cultural norms? This question is important because it helps to assess whether the client’s behavior is influenced by their cultural background and values, which may differ from those of the staff and other clients.
For example, some cultures may value privacy, modesty, or respect for elders more than others, and may avoid eye contact or social interaction as a sign of politeness or deference.
Understanding the client’s cultural norms can help to provide culturally sensitive and appropriate care.
Choice A is wrong because it assumes that the client’s behavior is caused by negative interactions with other clients, which may not be the case.
Choice B is wrong because it assumes that the client’s behavior is caused by hostile thoughts about others, which may not be the case.
Choice C is wrong because it assumes that the client’s behavior is caused by fear of others in the unit, which may not be the case.
These choices are not relevant to planning the client’s care and may reflect bias or stereotyping on the part of the staff.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today