A middle-aged school teacher complains of excessive tearing of the eyes every morning. Which assessment should the nurse perform next?
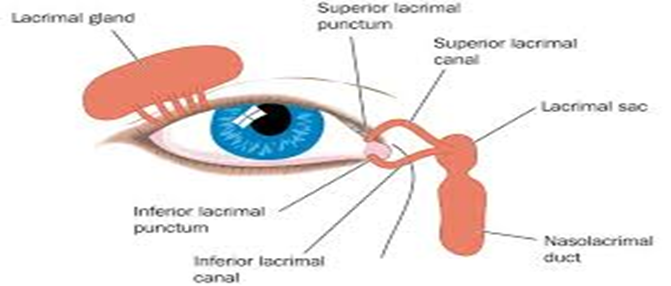
Assess the nasolacrimal sac
Inspect the palpebral conjunctiva
Test pupillary reaction to light
Perform the eye positions test
The Correct Answer is A
Choice A Reason:
The nasolacrimal sac is part of the tear drainage system. When a patient presents with excessive tearing, known as epiphora, it is important to assess for any obstruction in the lacrimal apparatus. The nasolacrimal sac can become blocked due to various reasons such as infection, inflammation, or structural abnormalities. Assessing this area can help determine if there is a blockage causing the tears to accumulate and overflow.
Choice B Reason:
Inspecting the palpebral conjunctiva is typically done if there is a complaint of eye pain or a sensation of a foreign body in the eye. While it is part of a comprehensive eye examination, it is not the first assessment to be performed for excessive tearing unless there are additional symptoms that suggest a problem with the conjunctiva.
Choice C Reason:
Testing the pupillary reaction to light is an assessment of the pupillary response and the function of the oculomotor nerve. This test is crucial when neurological issues are suspected or if there is a change in vision. However, it is not the primary assessment for excessive tearing without other associated symptoms.
Choice D Reason:
The eye positions test, which assesses eye muscle strength and cranial nerve function, is not necessary unless there are signs of problems with muscle strength, such as drooping. This test would not typically be the next step in assessing a patient with excessive tearing unless there are other indications of muscle or nerve impairment.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","C","D"]
Explanation
Choice A Reason:
Assessing vital signs is crucial for evaluating the client's responses to treatment. Changes in vital signs can indicate whether the body is responding positively or negatively to a treatment, allowing healthcare providers to adjust care plans accordingly. For example, a decrease in fever after administering antipyretics would suggest the treatment is effective.
Choice B Reason:
While carrying out orders from the healthcare provider is a responsibility of the nurse, it is not the primary reason for assessing vital signs. Vital signs are assessed to inform clinical decisions, not solely to fulfill orders. Therefore, this choice is not correct in the context of the importance of vital sign assessment.
Choice C Reason:
Monitoring risks for alterations in health is another key reason for assessing vital signs. Vital signs can serve as early indicators of health issues, such as the onset of an infection indicated by a rising temperature or cardiovascular problems suggested by changes in blood pressure or heart rate.
Choice D Reason:
Establishing a baseline is essential when assessing vital signs. It provides a reference point for future comparisons, which is important for detecting any deviations from the client's normal range. This helps in identifying potential health issues early and monitoring the progression of known conditions.
Correct Answer is B
Explanation
Choice A reason:
Discussing reactions to allergens typically focuses on environmental or food triggers that may cause allergic reactions. While it's important to understand a client's allergies, this topic is not closely related to alcohol use, which has different implications for health and lifestyle choices.
Choice B reason:
Asking about alcohol use naturally follows the discussion about cigarette smoking because both involve substance use and have potential health risks. It allows the nurse to transition smoothly from one lifestyle factor to another, which can impact the client's overall health. This approach also helps in creating a comprehensive picture of the client's habits that may contribute to or affect their current health status.
Choice C reason:
Reviewing current medications is an essential part of the health history, as it can reveal potential interactions with alcohol. However, it might be more appropriate to ask about alcohol use after discussing other lifestyle habits such as smoking, as they are more directly related. Once the client's substance use habits are established, the nurse can then discuss how these might interact with prescribed medications.
Choice D reason:
Asking about previous surgeries is important for understanding a client's medical history, but it is not directly related to the client's current lifestyle habits like alcohol use. Therefore, it would be more natural to ask about alcohol use in the context of other substance use discussions rather than after surgical history.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today