A female client is admitted with complaints of abdominal pain, loss of appetite, and a weight loss of 25 pounds (11 kg) in the last four months. During the admission assessment, the client tells the nurse that she has no interest in playing cards with her friends anymore and feels worthless most days. Which nursing problem should the nurse address first?
Anxiety as evidenced by abdominal complaints secondary to depression.
Imbalanced nutrition as evidenced by 25 pound (11 kg) weight loss in four months.
Chronic low self-esteem as evidenced by feelings of worthlessness.
Risk for self-directed violence as evidenced by feelings of hopelessness.
The Correct Answer is D
The client's statement of feeling worthless most days and having no interest in activities she previously enjoyed indicates a potential risk for self-directed violence, including self-harm or suicidal ideation. These signs are significant and require immediate attention and intervention by the nurse.
Assessing and addressing the client's risk for self-directed violence is of utmost importance to ensure her safety and well-being. The nurse should initiate a thorough assessment of the client's mental health, including assessing for any suicidal ideation, intent, or plans. It is crucial to establish a supportive and non-judgmental environment for the client to express her feelings and concerns.
The nurse should collaborate with the healthcare team to develop an appropriate care plan that may involve interventions such as close observation, involving a mental health professional, implementing safety measures, and providing emotional support.
While addressing other nursing problems, such as anxiety, imbalanced nutrition, and chronic low self-esteem, is important, the immediate concern is the client's risk for self-directed violence due to her feelings of hopelessness.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Administering a large volume of medication in a single injection is not recommended for infants as it can lead to discomfort, tissue trauma, and potential complications such as muscle fibrosis or nerve injury. Dividing the medication into two injections with volumes under 1 mL is a common practice for infants and can help minimize discomfort and complications.
In addition, the nurse should select an appropriate needle size and injection site based on the infant's size and age. A 22 gauge 1 1/2 inch (3.8 cm) needle is too large for an infant and may cause discomfort and tissue damage. The nurse should use a smaller gauge needle and choose an appropriate injection site, such as the vastus lateralis muscle in the thigh or the dorsogluteal muscle in the buttocks, based on the infant's age and size.
Finally, administering an injection into the deltoid muscle is not recommended for infants as this muscle is not fully developed until later in childhood. Using a quick dart-like motion to inject into the dorsogluteal site is also not recommended as it can cause tissue damage and discomfort. Instead, the nurse should use a slow, steady technique to administer the injection while ensuring the infant is held securely by the parent or another caregiver.
Correct Answer is A
Explanation
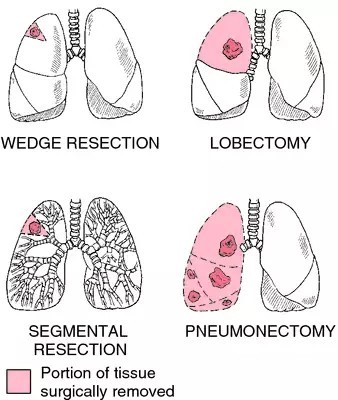
Following a pneumonectomy, it is important for the client to gradually resume normal activities and engage in social interactions. Encouraging family gatherings can provide emotional support, facilitate social connections, and help reduce feelings of isolation that the client may be experiencing.
While it is generally important for clients who have undergone a pneumonectomy to take precautions to reduce the risk of respiratory infections, such as avoiding crowded places and individuals with respiratory infections, completely avoiding social contact for several weeks is not necessary or realistic in most cases. It is essential to find a balance between protecting the client's health and promoting their emotional well-being and social integration.
Wearing a face mask during family events may not be necessary unless there is a specific concern about respiratory infections. The nurse can educate the client about the importance of good hand hygiene and avoiding close contact with individuals who are actively ill with respiratory infections.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today