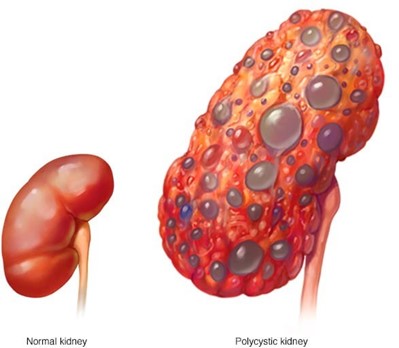
A client is being treated for chronic kidney disease (CKD). On examination, the client has an elevated blood pressure (BP) and is exhibiting changes in mental status. Which intervention in the plan of care should the practical nurse (PN) implement?
Use a cushion when sitting.
Perform range of motion exercises.
Document abdominal girth.
Weigh every morning.
The Correct Answer is D
This is the best intervention for the PN to implement because it monitors the client's fluid status and helps detect fluid overload, which can cause hypertension and neurological changes. The PN should weigh the client at the same time, on the same scale, and with the same clothing every day.
A. Using a cushion when sitting is not a priority intervention for this client and may not address the BP or mental status issues.
B. Performing range of motion exercises is not a priority intervention for this client and may not address the BP or mental status issues.
C. Documenting abdominal girth is not a priority intervention for this client and may not be an accurate indicator of fluid status.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
This is the best action that describes the responsibility of the PN because it ensures that the client has given informed consent for the invasive examination and that the consent form is valid and documented. The PN should verify that the provider has explained the examination, its risks and benefits, and alternative options to the client and that the client has agreed to proceed.
Correct Answer is A
Explanation
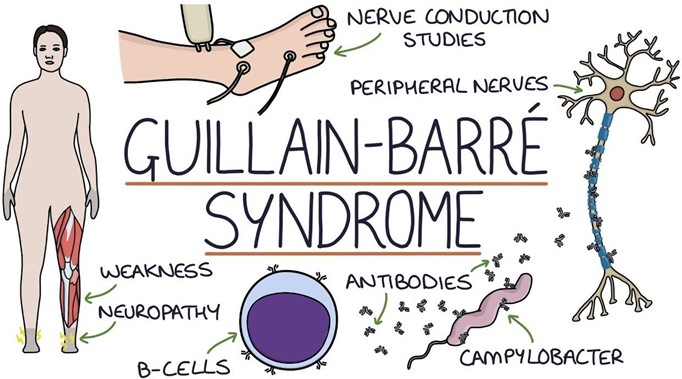
This is the finding that the PN should report to the charge nurse because it indicates a possible complication of Guillain-Barre syndrome, which is autonomic dysfunction. This can affect the cardiac, respiratory, and gastrointestinal systems and cause life-threatening problems such as arrhythmias, hypotension, or respiratory failure. The PN should monitor the client's vital signs closely and report any abnormal changes.
B. Profuse diaphoresis is not a priority finding and may be related to other factors such as fever, anxiety, or medication side effects.
C. Lower leg weakness is an expected finding in Guillain-Barre syndrome and does not need to be reported unless it progresses rapidly or affects the respiratory muscles.
D. Full facial flushing is not a priority finding and may be related to other factors such as vasodilation, inflammation, or medication side effects.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today