Which finding(s) should the nurse expect to assess in a 16-year-old client diagnosed with cystic fibrosis admitted to the hospital for decreased results on pulmonary function tests (PFTs)?
Meconium ileus.
Blood-streaked sputum.
Clear breath sounds bilaterally.
Dyspnea.
The Correct Answer is B
Choice A rationale:
Meconium ileus is a concern in newborns with cystic fibrosis due to thick meconium, which can cause intestinal obstruction. At 16 years old, this complication is not relevant to the client's current condition.
Choice B rationale:
Blood-streaked sputum is a likely finding in a 16-year-old with cystic fibrosis and decreased pulmonary function. Cystic fibrosis leads to mucus accumulation and lung infections, which can cause blood vessels to rupture, resulting in blood-streaked sputum.
Choice C rationale:
Clear breath sounds bilaterally indicate healthy lung function, which is not expected in a client with cystic fibrosis and decreased PFT results. Breath sounds are likely to be diminished due to mucus accumulation.
Choice D rationale:
Dyspnea, or difficulty breathing, is a common symptom in clients with cystic fibrosis and decreased pulmonary function. However, the question asks about the expected findings that the nurse should assess, not a symptom that the client might report.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale:
Allowing the patient to stay in the chosen position might not be the best approach, as the child's preference might not align with therapeutic considerations for managing status asthmaticus.
Choice B rationale:
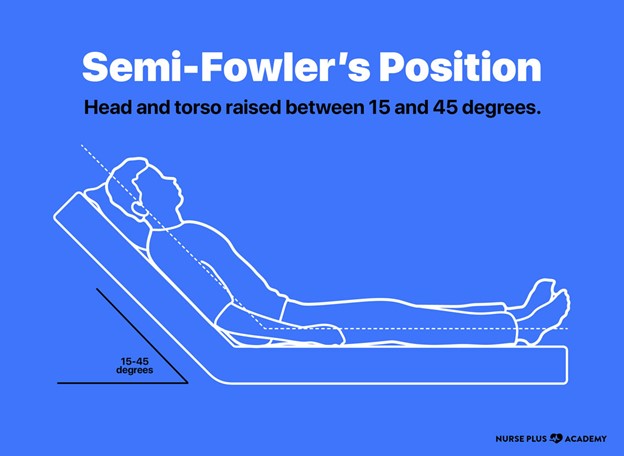
Semi-Fowler's position, with the head of the bed elevated, promotes improved lung expansion and easier breathing for patients with respiratory distress. Explaining the rationale behind this position to the child helps them understand its therapeutic benefits, encouraging compliance.
Choice C rationale:
Demonstrating various positions could confuse the child and delay appropriate intervention. A clear explanation of the preferred position is more effective in this critical situation.
Choice D rationale:
Removing pillows might be counterproductive, as elevating the head of the bed is beneficial for respiratory distress. This choice contradicts the therapeutic goal.
Correct Answer is B
Explanation
Choice A rationale:
Strict isolation should begin immediately after exposure. This choice is incorrect because chickenpox does not require strict isolation immediately after exposure. The incubation period of chickenpox is about 10-21 days, during which communicability has not yet begun.
Choice B rationale:
Communicability begins prior to the eruption of lesions. This choice is correct. Chickenpox is highly contagious, and individuals can transmit the virus to others even before the characteristic skin lesions appear. This understanding is crucial for appropriate room assignment to prevent the spread of the virus to other patients.
Choice C rationale:
Strict isolation should begin as soon as the skin lesions erupt. This choice is incorrect. While isolation precautions are necessary for patients with active chickenpox lesions, waiting until the lesions erupt is not sufficient to prevent transmission, as communicability starts before this stage.
Choice D rationale:
Communicability begins 14 days after exposure. This choice is incorrect. The correct timing for the onset of communicability is much earlier than 14 days after exposure. Waiting until this point for isolation would not effectively prevent transmission.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today