When preparing to apply a scheduled fentanyl transdermal patch, the nurse notes that the previously applied patch is intact on the client’s upper back and the client denies pain. Which action should the nurse take?
Place the patch on the client’s shoulder and leave both patches in place for 12 hours.
Remove the patch and consult with the healthcare provider about the client’s pain resolution.
Apply the new patch in a different location after removing the original patch.
Administer an oral analgesic and evaluate its effectiveness before applying the new patch.
The Correct Answer is C
Choice A reason:
Placing the new patch on the client’s shoulder and leaving both patches in place for 12 hours is not recommended. Fentanyl patches are designed to be used one at a time, and overlapping patches can lead to an overdose due to excessive absorption of the medication1. The standard practice is to remove the old patch before applying a new one.
Choice B reason:
Removing the patch and consulting with the healthcare provider about the client’s pain resolution is a cautious approach. However, it is not necessary to consult the healthcare provider if the client denies pain and the patch is due for replacement. The nurse should follow the standard protocol for patch replacement.
Choice C reason:
Applying the new patch in a different location after removing the original patch is the correct action. This ensures that the medication is delivered effectively while preventing skin irritation and potential overdose. The new patch should be placed on a different area of intact skin to allow the previous site to recover.
Choice D reason:
Administering an oral analgesic and evaluating its effectiveness before applying the new patch is not appropriate in this scenario. The client is already receiving pain management through the transdermal patch, and additional oral analgesics are not necessary unless there is breakthrough pain. The focus should be on proper patch replacement
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: Hypercholesterolemia, or high cholesterol, is not a primary concern when prescribing methylphenidate. While managing cholesterol levels is important for overall cardiovascular health, it does not directly interact with the administration of methylphenidate.
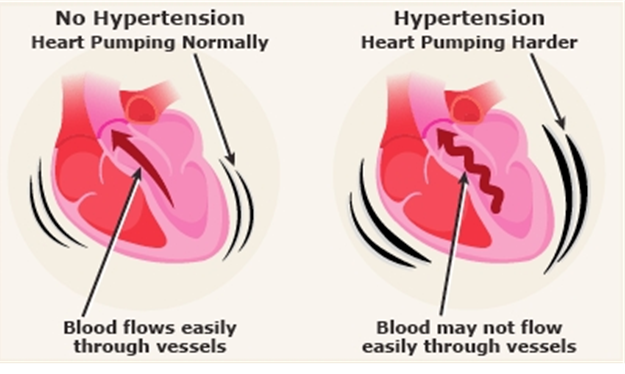
Choice B reason: Hypertension, or high blood pressure, is a critical condition to review before administering methylphenidate. Methylphenidate can increase blood pressure and heart rate, potentially exacerbating pre-existing hypertension. Monitoring and managing blood pressure is essential to prevent complications such as stroke or heart attack.
Choice C reason: Diabetes mellitus is important to manage, but it is not directly affected by methylphenidate. While some medications can influence blood sugar levels, methylphenidate primarily affects the central nervous system and cardiovascular system.
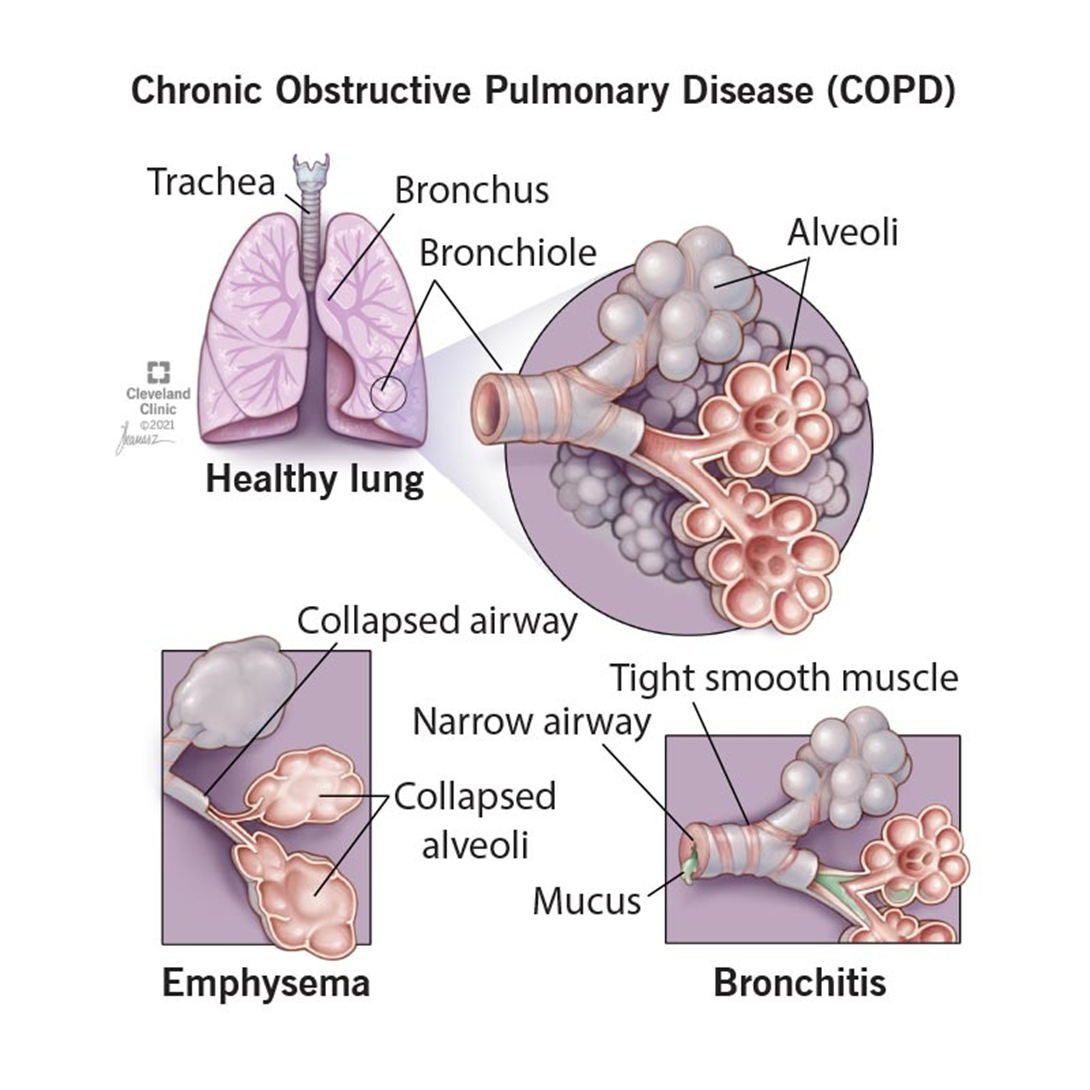
Choice D reason: Bronchitis, an inflammation of the bronchial tubes, is not a primary concern with methylphenidate use. Although respiratory conditions should be managed appropriately, they do not typically interact with the effects of methylphenidate.
Correct Answer is D
Explanation
Choice A reason:
Rinsing the mouth after each use of an inhaler is a recommended practice, especially for inhalers containing corticosteroids, to prevent oral thrush and other side effects. Although ipratropium is not a corticosteroid, rinsing the mouth can still help reduce any potential irritation or unpleasant taste.
Choice B reason:
Storing the medication at room temperature is appropriate for most inhalers, including ipratropium2. This ensures the medication remains effective and safe to use. It is important to keep the inhaler away from extreme temperatures and direct sunlight.
Choice C reason:
Attaching a spacer device to the inhaler can be beneficial, especially for patients who have difficulty coordinating the timing of inhalation with the activation of the inhaler. A spacer helps ensure that more medication reaches the lungs rather than being deposited in the mouth or throat.
Choice D reason:
Priming the inhaler with 7 pumps is excessive. Typically, ipratropium inhalers require priming with only 2 to 4 sprays before the first use or if the inhaler has not been used for a few days. Over-priming can waste medication and may indicate that the client needs additional instruction on proper inhaler use.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today