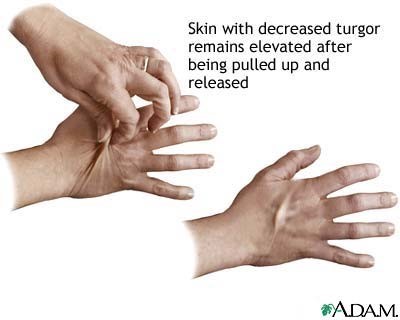
The nurse is performing a head-to-toe assessment on a patient. The nurse uses their thumb and first finger to lift or pinch a fold of skin under the clavicle to check for skin turgor. Which of the following findings would be considered normal for this assessment?
Skin fold is difficult to lift/pinch.
Skin fold is released and an indentation of 2 mm remains.
Skin fold returns to its usual shape quickly when released.
Skin fold returns to its usual shape slowly when released.
The Correct Answer is C
The correct answer is choice C: Skin fold returns to its usual shape quickly when released. When assessing skin turgor, the nurse is checking for the elasticity and hydration of the skin. In a normal assessment, when the skin fold is lifted or pinched, it should return to its usual shape quickly when released. This indicates good skin turgor, which is an indication of proper hydration. If the skin fold is difficult to lift or pinch (choice A), this indicates poor skin turgor and possible dehydration. If an indentation of 2 mm remains after releasing the skin fold (choice B), this indicates poor skin turgor and possible dehydration. If the skin fold returns to its usual shape slowly when released (choice D), this may indicate a decrease in skin elasticity and possible dehydration.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
The correct answer is choice C, face. When beginning a complete bed bath, the nurse should first wash the client's face, followed by the arms, chest, abdomen, legs, perineal area, back, and then feet. Washing the face first is important to promote client comfort and hygiene, and also sets a positive tone for the rest of the bath. Additionally, washing the face before the perineal area helps to prevent cross-contamination of bacteria from the perineal area to the face.
Correct Answer is C
Explanation
Answer and Explanation
The correct answer is choice C, Read back the order to the physician.
After obtaining the physician's order over the phone, the nurse should read back the order to the physician to confirm accuracy and prevent medication errors.
This process ensures that the order is correctly transcribed and the right medication, dose, and route are given to the patient. Calling the pharmacy to check medication availability is not the nurse's responsibility, and initiating the prescription and administering the medication is inappropriate without confirming the order with the physician. Drawing up the medication into an appropriately labeled syringe before confirming the order with the physician is also inappropriate and can lead to medication errors. Therefore, reading back the order to the physician is the most appropriate action for the nurse to take.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today