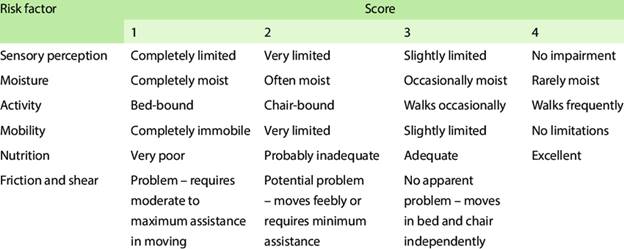
The nurse is completing a skin risk assessment using the Braden Scale. The patient has slight sensory impairment, has skin that is rarely moist, walks occasionally, and has slightly limited mobility, along with excellent intake of meals and no apparent problem with friction and shearing. Which score will the nurse document for this patient?
23
15
17
20
The Correct Answer is D
- Sensory perception: Slightly limited (score of 3)
- Moisture: Rarely moist (score of 4)
- Activity: Walks occasionally (score of 3)
- Mobility: Slightly limited (score of 3)
- Nutrition: Excellent intake (score of 4)
- Friction and shear: No apparent problem (score of 3)
Adding these scores together: 3 + 4 + 3 + 3 + 4 + 3 = 20
Therefore, the nurse should document a score of 20 for this patient.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. "I will treat all the family members to be on the safe side." Treatment is only recommended for individuals who have active lice or close, prolonged contact with the infected child. Treating everyone unnecessarily may lead to overuse of medications.
B. "My child must be free from nits before returning to school." The CDC and AAP do not recommend "no-nit" policies, as nits alone do not indicate active infestation. Children can return to school after appropriate treatment begins.
C. "Toys that can't be dry cleaned or washed must be thrown out." Non-washable items should be sealed in a plastic bag for 2 weeks to kill lice, rather than being thrown away.
D. "All recently used clothing, bedding, and towels must be washed in hot water." Lice and nits can survive on fabric surfaces, so washing clothing, bedding, and towels in hot water (≥130°F/54°C) and drying on high heat is recommended to eliminate them.
Correct Answer is C
Explanation
A. Stage I Pressure Ulcer: A Stage III pressure ulcer does not regress to a Stage I as it heals. It retains its original staging classification.
B. Stage III Pressure Ulcer: While the ulcer was originally Stage III, documenting it this way without specifying healing progress does not accurately reflect its current condition.
C. Healing Stage III Pressure Ulcer: Pressure ulcers are documented at their worst stage, even as they heal. The correct terminology includes "healing" to show improvement.
D. Healing Stage II Pressure Ulcer: A Stage III ulcer does not become a Stage II ulcer as it heals; instead, it is called a healing Stage III pressure ulcer.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today