During a skin inspection at the outpatient clinic, the nurse notices patches of thick, red skin with silvery scales on the client's elbows and knees. What skin abnormality does the nurse suspect?
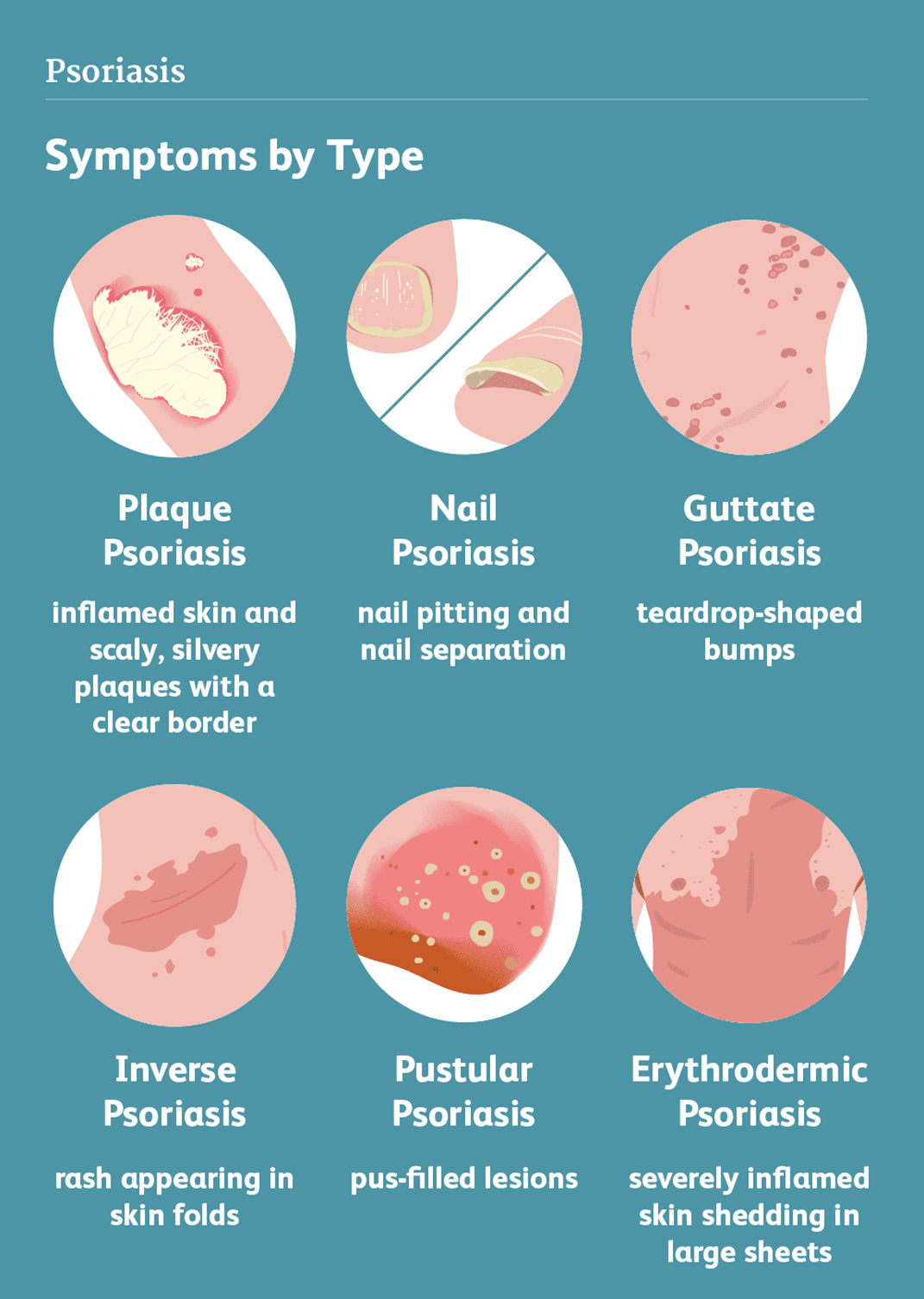
Psoriasis
Rosacea
Scabies
Stasis dermatitis
The Correct Answer is A
Choice A reason: Psoriasis is a skin abnormality that causes patches of thick, red skin with silvery scales, usually on the elbows, knees, scalp, lower back, or genitals. Psoriasis is a chronic, inflammatory, autoimmune condition that affects the life cycle of skin cells, causing them to build up rapidly on the surface of the skin. Psoriasis can cause itching, burning, pain, or bleeding.
Choice B reason: Rosacea is a skin abnormality that causes redness, flushing, swelling, or pimples, usually on the face, especially the cheeks, nose, chin, or forehead. Rosacea is a chronic, inflammatory, vascular condition that affects the blood vessels and sebaceous glands of the skin. Rosacea can cause sensitivity, stinging, or dryness.
Choice C reason: Scabies is a skin abnormality that causes small, red bumps, blisters, or burrows, usually on the hands, wrists, feet, ankles, or genitals. Scabies is a contagious, parasitic infection that is caused by tiny mites that burrow into the skin and lay eggs. Scabies can cause intense itching, especially at night.
Choice D reason: Stasis dermatitis is a skin abnormality that causes swelling, redness, scaling, or ulcers, usually on the lower legs or ankles. Stasis dermatitis is a chronic, inflammatory condition that results from poor blood circulation in the veins of the legs, causing fluid to leak into the surrounding tissues. Stasis dermatitis can cause pain, itching, or infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Primary intention is the correct answer, because it is the type of wound healing that occurs when the wound edges are approximated and closed with sutures, staples, or glue. Primary intention is the fastest and most effective way of wound healing, as it minimizes tissue loss, infection, and scarring.
Choice B reason: Secondary intention is not the correct answer, because it is the type of wound healing that occurs when the wound edges are not approximated and left open to heal by granulation, contraction, and epithelialization. Secondary intention is the slowest and least effective way of wound healing, as it results in more tissue loss, infection, and scarring.
Choice C reason: Tertiary intention is not the correct answer, because it is the type of wound healing that occurs when the wound edges are initially left open and then closed with sutures, staples, or glue after a period of time. Tertiary intention is a delayed form of primary intention, and it is used when the wound is contaminated, infected, or requires drainage.
Choice D reason: Binary intention is not the correct answer, because it is not a real term for wound healing. Binary intention is a madeup term that does not describe any specific process or outcome of wound healing.
Correct Answer is D
Explanation
Choice A reason: This is not the priority assessment, but it is an important assessment for a client with a femur fracture. Pain is the unpleasant sensation that results from tissue damage or inflammation. Pain can affect the client's physical and psychological wellbeing and interfere with their recovery. The nurse should assess the client's pain level, location, quality, and duration using a valid and reliable pain scale. The nurse should also provide pain relief measures, such as medication, ice, elevation, or distraction, as ordered and as needed.
Choice B reason: This is not the priority assessment, but it is a relevant assessment for a client with a femur fracture. Medication history is the record of the drugs that the client is currently taking or has taken in the past, including prescription, overthecounter, herbal, or recreational drugs. Medication history can help the nurse identify any potential drug interactions, allergies, or contraindications that may affect the client's treatment and recovery. The nurse should ask the client about their medication history and document it accurately and completely.
Choice C reason: This is not the priority assessment, but it is a helpful assessment for a client with a femur fracture. Socioeconomic status is the measure of the client's income, education, occupation, and social class. Socioeconomic status can influence the client's access to health care, ability to afford treatment, compliance with therapy, and support system. The nurse should assess the client's socioeconomic status and provide appropriate referrals, resources, or assistance as needed.
Choice D reason: This is the priority assessment for a client with a femur fracture. Pedal pulses are the pulses that can be felt in the feet, such as the dorsalis pedis or the posterior tibial pulse. Pedal pulses can indicate the blood flow and perfusion to the lower extremities, which can be compromised by a femur fracture. A femur fracture can cause bleeding, swelling, or pressure that can reduce or obstruct the blood supply to the feet, leading to ischemia, necrosis, or gangrene. The nurse should assess the client's pedal pulses regularly and report any changes, such as absent, weak, or thready pulses. The nurse should also monitor the client's skin color, temperature, sensation, and movement in the feet.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today