An older client recently transferred to a rehabilitation facility after aortic valve replacement surgery is experiencing anxiety and difficulty adjusting to the transition. The healthcare provider prescribes an antidepressant and a mild sedative for sleep. Which intervention is most important for the nurse to include in the client's plan of care?
Obtain a blood pressure reading before the client gets out of bed.
Monitor and record the client's urinary output every day.
Provide the client with teaching regarding a cardiac diet.
Assess the client's vital signs every 4 hours when awake.
The Correct Answer is A
Choice A: Obtain a blood pressure reading before the client gets out of bed. This is the most important intervention, as it can prevent or detect orthostatic hypotension, which is a drop in blood pressure when changing position from lying to standing. Orthostatic hypotension can cause dizziness, fainting, or falls, and it can be caused by medications, dehydration, or cardiac problems.
Choice B: Monitor and record the client's urinary output every day. This is not the most important intervention, as it does not address the client's anxiety or adjustment issues. The urinary output should be monitored for signs of fluid balance, kidney function, or infection, but it is not a priority for this client.
Choice C: Provide the client with teaching regarding a cardiac diet. This is not the most important intervention, as it does not address the client's anxiety or adjustment issues. The cardiac diet should be taught to promote heart health, lower cholesterol, and reduce sodium intake, but it is not a priority for this client.
Choice D: Assess the client's vital signs every 4 hours when awake. This is not the most important intervention, as it does not address the client's anxiety or adjustment issues. The vital signs should be assessed for signs of infection, pain, or hemodynamic instability, but they are not a priority for this client.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A: Monitoring indwelling urinary catheter and measure strict intake and output is not an action that the nurse should immediately take, as this is not relevant or urgent for a client who may have had a stroke. This is a distractor choice.
Choice B: Keeping the bed in the lowest position and initiating seizure and fall precautions is not an action that the nurse should immediately take, as this is a preventive measure that does not address the acute problem of impaired cerebral perfusion. This is another distractor choice.
Choice C: Starting two large bore IV catheters and reviewing inclusion criteria for IV fibrinolytic therapy is an action that the nurse should immediately take, as this can prepare the client for potential administration of tissue plasminogen activator (tPA., which can dissolve blood clots and restore blood flow to the brain if given within 4.5 hours of stroke onset. Therefore, this is the correct choice.
Choice D: Maintaining elevated positioning of the dependent joints on affected side is not an action that the nurse should immediately take, as this can worsen edema and impair circulation in the affected limbs. The recommended position is to keep them at or below heart level. This is another distractor choice.
Correct Answer is A
Explanation
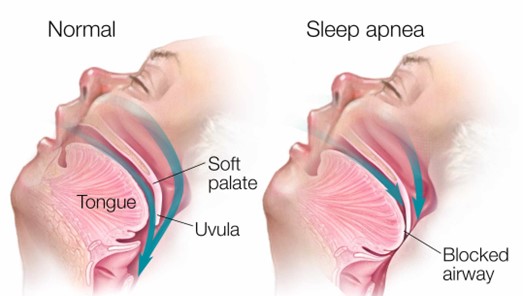
Choice B reason: Elevating the head of the bed to a 45-degree angle is not a sufficient intervention for the nurse to implement before leaving the client. Elevating the head of the bed can help reduce snoring and improve breathing by preventing the tongue and soft palate from falling back and obstructing the airway. However, it may not be enough to prevent apnea episodes in clients with obstructive sleep apnea, especially if they have other risk factors such as obesity, enlarged tonsils, or nasal congestion. The nurse should also use other interventions such as a positive airway pressure device, weight loss, or surgery.
Choice C reason: Removing dentures or other oral appliances is not a relevant intervention for the nurse to implement before leaving the client. Dentures or other oral appliances are devices that replace missing teeth or improve dental alignment. They may help improve speech, chewing, and appearance, but they do not have a direct impact on obstructive sleep apnea. The nurse should instruct the client to remove dentures or other oral appliances before going to bed to prevent discomfort, infection, or damage.
Choice D reason: Lifting and locking the side rails in place is not a necessary intervention for the nurse to implement before leaving the client. Side rails are bars that attach to the sides of the bed frame to prevent falls or injuries. They may provide safety and security for some clients, but they may also pose risks such as entrapment, strangulation, or agitation. The nurse should assess the need for side rails on an individual basis and consider alternative measures such as bed alarms, low beds, or floor mats.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today