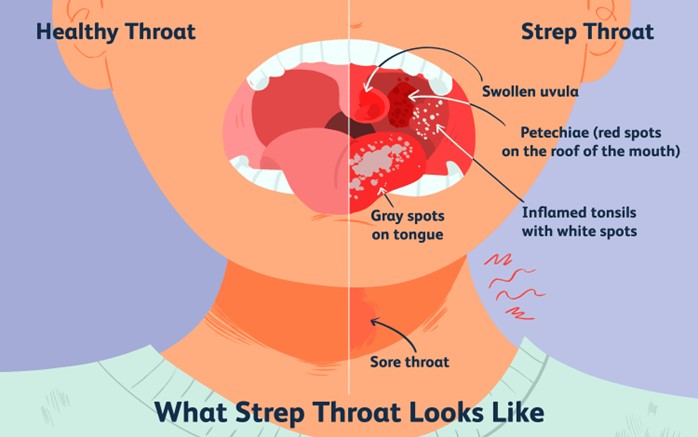
A nurse is reinforcing teaching with a client who has streptococcal pharyngitis. Which of the following actions is appropriate for the nurse to include in the plan of care?
Place the client in a negative airflow room.
Implement droplet precautions.
Place the client on a fluid restriction.
Obtain a throat culture after the initial dose of antibiotics.
The Correct Answer is B
Choice A reason: This is not an appropriate action for this client because placing them in a negative airflow room is indicated for clients who have airborne infections, such as tuberculosis or measles, that can spread through small particles that remain suspended in air. Streptococcal pharyngitis, also known as strep throat, is caused by bacteria that spread through large respiratory droplets that fall within 3 feet from source.
Choice B reason: This is an appropriate action for this client because implementing droplet precautions can prevent transmission of streptococcal pharyngitis to others by contact with respiratory secretions or contaminated objects. The nurse should wear a surgical mask when entering the client's room and instruct visitors to do so as well. The nurse should also place a mask on the client when transporting them outside their room.
Choice C reason: This is not an appropriate action for this client because placing them on a fluid restriction can cause dehydration and impair mucosal healing. The nurse should encourage the client to drink plenty of fluids, such as water, tea, or broth, to soothe the throat and prevent dryness.
Choice D reason: This is not an appropriate action for this client because obtaining a throat culture after the initial dose of antibiotics can affect the accuracy of the test results and delay diagnosis and treatment. The nurse should obtain a throat culture before starting antibiotics to confirm the presence of streptococcal bacteria and guide antibiotic therapy.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: This is not an appropriate response because it implies that the nurse does not acknowledge or validate the partner's feelings. The nurse should provide emotional support and education to the partner about the normal changes that occur at the end of life.
Choice B reason: This is not an appropriate response because it may cause more distress and fatigue to the client and the partner. The nurse should respect the client's need for rest and allow them to sleep as much as they want.
Choice C reason: This is not an appropriate response because it may interfere with the client's comfort and quality of life. The nurse should avoid unnecessary interventions and medications that may have adverse effects or cause more harm than benefit.
Choice D reason: This is the correct answer because it shows empathy and compassion to the partner and the client. The nurse should encourage the partner to spend time with the client and offer nonverbal communication such as holding hands, stroking hair, or playing soft music.
Correct Answer is B
Explanation
Choice A reason: This is not a correct statement because applying the TENS unit at least 6 inches from the actual site of pain can reduce its effectiveness and cause discomfort or irritation to other areas of the skin. The nurse should instruct the client to apply the electrodes directly over or around the site of pain and follow the provider's instructions regarding placement.
Choice B reason: This is a correct statement because adjusting the TENS unit until feeling a tingling sensation can indicate that it is delivering an adequate amount of electrical stimulation to block pain signals from reaching the brain. The nurse should instruct the client to turn on the TENS unit and increase the intensity gradually until feeling a strong but comfortable tingling sensation.
Choice C reason: This is not a correct statement because charging the TENS unit for 2 hours each day can vary depending on the type and model of the device and its battery life. The nurse should instruct the client to follow the manufacturer's instructions regarding charging and maintenance of the TENS unit and check its power level before each use.
Choice D reason: This is not a correct statement because administering a continuous dose of pain medication is not a function of the TENS unit, which does not deliver any drugs or chemicals into the body. The nurse should instruct the client that the TENS unit works by sending mild electrical impulses through electrodes attached to pads that are placed on the skin.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today