A nurse cares for a patient who has a serum potassium of 7.5 mEq/L and is exhibiting cardiovascular changes. Which should the nurse implement first?
Provide a heart healthy low potassium diet
Prepare to administer sodium polystyrene sulfate 15g by mouth
Prepare the patient for hemodialysis treatment
Prepare to administer dextrose 20% and 10 units of regular insulin IV push
The Correct Answer is D
A. Provide a heart-healthy low-potassium diet:
While a heart-healthy low-potassium diet is essential for managing chronic hyperkalemia and preventing future occurrences, it is not the first intervention to implement in a patient with a serum potassium level of 7.5 mEq/L and exhibiting cardiovascular changes. The effects of dietary changes on serum potassium levels are gradual and may take days to have a significant impact. In an acute situation like this, immediate interventions are needed to rapidly lower potassium levels and address the associated cardiovascular risks.
B. Prepare to administer sodium polystyrene sulfate 15g by mouth:
Sodium polystyrene sulfate is a medication used to exchange sodium for potassium in the gastrointestinal tract, effectively lowering serum potassium levels over hours to days. While it is a valid treatment for hyperkalemia, its onset of action is not immediate enough to address the urgent cardiovascular changes seen in severe hyperkalemia. Therefore, it is not the first-line intervention in this scenario.
C. Prepare the patient for hemodialysis treatment:
Hemodialysis is an effective method for rapidly lowering serum potassium levels in cases of severe hyperkalemia. However, it is a more invasive and time-consuming procedure that requires preparation, including vascular access and dialysis setup. It is typically reserved for situations where other interventions have failed or in patients with severe or refractory hyperkalemia. In the context of this scenario, where the patient has a serum potassium level of 7.5 mEq/L and is exhibiting cardiovascular changes, hemodialysis may be considered if initial interventions are not successful, but it is not the first action to implement.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["E"]
Explanation
A. Increased pulse rate:
This is a common manifestation of fluid overload. Excess fluid volume can lead to an increase in cardiac output, causing the heart to pump faster and resulting in an increased pulse rate.
B. Decreased blood pressure:
Fluid overload typically leads to increased blood volume, which can initially cause an increase in blood pressure. However, as fluid overload progresses, it can lead to fluid redistribution, venous congestion, and decreased systemic vascular resistance, ultimately resulting in decreased blood pressure.
C. Skeletal muscle weakness:
Skeletal muscle weakness is not a direct manifestation of fluid overload. It is more commonly associated with electrolyte imbalances, such as hypokalemia or hypomagnesemia, which can occur as a consequence of fluid shifts but are not specific to fluid overload itself.
D. Warm and pink skin:
Warm and pink skin is not typically associated with fluid overload. Instead, it is more indicative of adequate tissue perfusion and oxygenation. In fluid overload, skin changes may include edema, cool and clammy skin due to venous congestion, or signs of skin breakdown in areas of pressure.
E. Distended neck veins:
Distended neck veins, specifically jugular venous distention (JVD), are commonly seen in patients with fluid overload, especially if there is right-sided heart failure or increased central venous pressure. JVD is a result of increased venous return to the heart due to fluid accumulation.
Correct Answer is B
Explanation
A. Loose connective tissue:
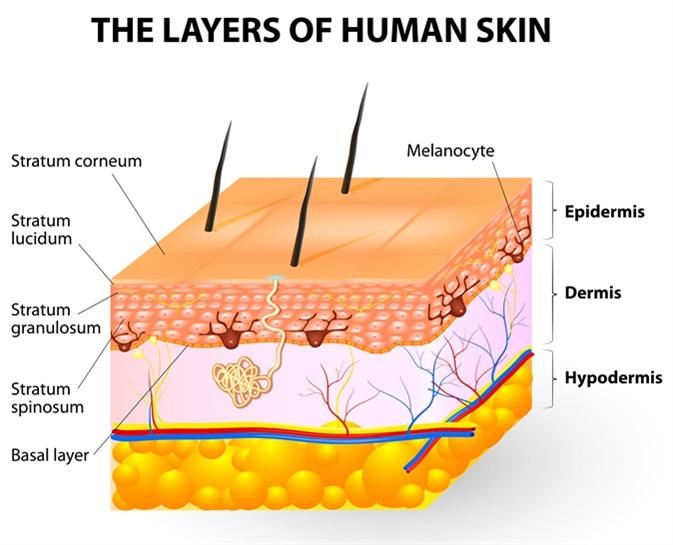
Melanocytes are not typically found in loose connective tissue. Their primary location is within the epidermis, specifically in the basal layer, where they interact with keratinocytes to produce melanin and contribute to skin color. Loose connective tissue contains collagen and elastin fibers, as well as fibroblasts, but it does not house melanocytes.
B. Epidermis:
This is the correct answer. Melanocytes are primarily located in the basal layer of the epidermis, which is the deepest layer of the epidermis. These cells produce melanin, a pigment that helps protect the skin from UV radiation and determines skin color. Melanocytes are interspersed among keratinocytes in the epidermis and transfer melanin to keratinocytes to provide skin pigmentation.
C. Dermis:
The dermis is the layer of skin beneath the epidermis and consists of connective tissue, blood vessels, nerves, hair follicles, and sweat glands. While the dermis plays a crucial role in supporting and nourishing the epidermis, melanocytes are not primarily located in the dermis. They are confined to the basal layer of the epidermis.
D. Superficial fascia:
The superficial fascia, also known as the subcutaneous tissue or hypodermis, lies beneath the dermis and consists of adipose (fat) tissue and connective tissue. It provides insulation, energy storage, and cushioning for underlying structures. However, melanocytes are not typically found in the superficial fascia. They are restricted to the epidermis, specifically the basal layer, where they carry out their function of melanin production.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today