A community health nurse is providing screening for lipid disorders. Which of the following is the primary goal of this activity?
Early detection of disease
Client enrollment in prevention programs
Promotion of appropriate lifestyle changes
Identification of family history of medical problems
The Correct Answer is A
Choice A reason: Early detection of disease is the primary goal of screening for lipid disorders, as it can identify clients who are at risk of developing cardiovascular diseases, such as coronary artery disease, stroke, or peripheral artery disease. Lipid disorders are abnormal levels of cholesterol or triglycerides in the blood, which can lead to plaque buildup in the arteries and reduce blood flow to the heart, brain, or limbs. Screening for lipid disorders can help diagnose and treat these conditions before they cause serious complications.
Choice B reason: Client enrollment in prevention programs is not the primary goal of screening for lipid disorders, although it is a beneficial outcome. Prevention programs are interventions that aim to reduce the risk factors or prevent the onset of diseases. Client enrollment in prevention programs may be a result of screening for lipid disorders, as clients who have abnormal lipid levels may be referred to programs that offer education, counseling, medication, or lifestyle modification.
Choice C reason: Promotion of appropriate lifestyle changes is not the primary goal of screening for lipid disorders, although it is a beneficial outcome. Lifestyle changes are behaviors that can improve health and well-being, such as eating a balanced diet, exercising regularly, quitting smoking, or managing stress. Promotion of appropriate lifestyle changes may be a result of screening for lipid disorders, as clients who have abnormal lipid levels may be advised to adopt healthier habits to lower their cholesterol or triglycerides.
Choice D reason: Identification of family history of medical problems is not the primary goal of screening for lipid disorders, although it is a beneficial outcome. Family history of medical problems is a genetic or environmental factor that can increase the likelihood of developing certain diseases. Identification of family history of medical problems may be a result of screening for lipid disorders, as clients who have abnormal lipid levels may be asked to provide information about their relatives' health conditions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
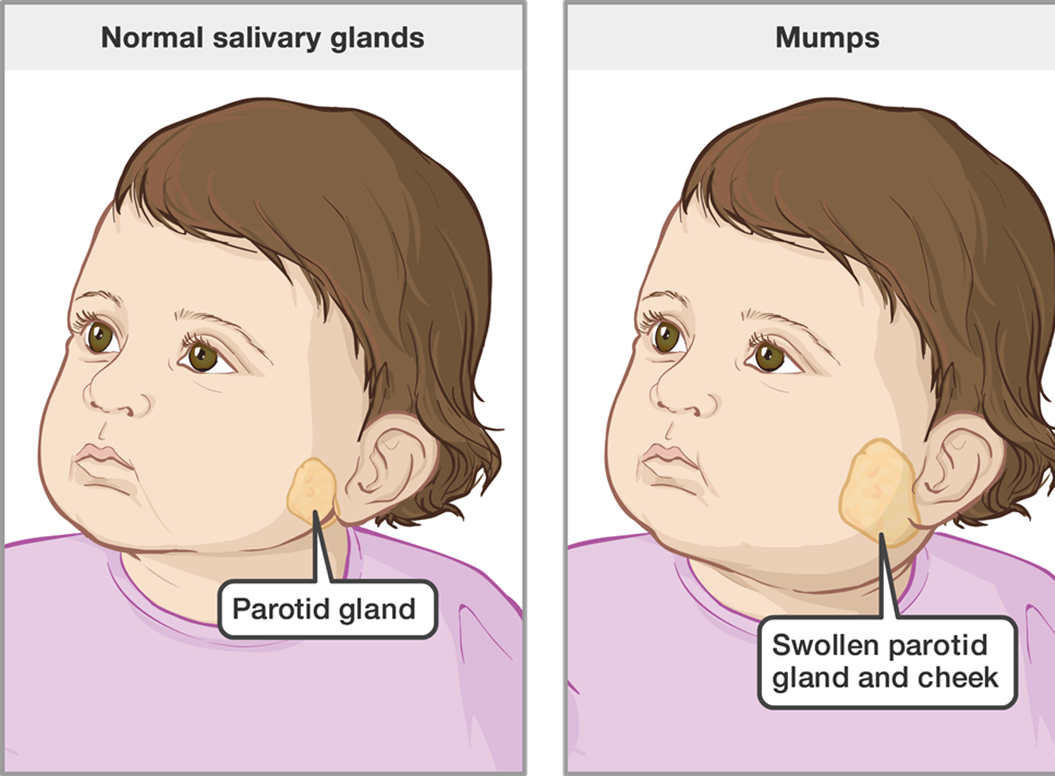
Choice A reason: The vaccine is not the host, as it is not a living organism that can be infected by the virus. The vaccine is a preventive measure that can reduce the risk of contracting mumps by stimulating the immune system to produce antibodies against the virus.
Choice B reason: The virus is not the host, as it is the agent that causes the disease. The virus is a microscopic particle that can only replicate inside the cells of a living host.
Choice C reason: The school is not the host, as it is the environment that facilitates the transmission of the virus. The school is a place where many children gather and interact, which increases the exposure and contact with the virus.
Choice D reason: The children are the host, as they are the living organisms that can be infected by the virus. The children are susceptible to the virus because they may not have been vaccinated or have not developed immunity from previous exposure. The children can also spread the virus to others through respiratory droplets or saliva.
Correct Answer is A
Explanation
Choice A reason:This is a correct recommendation. The American Academy of Ophthalmology advises adults aged 40–64 to have a comprehensive eye exam every 2 years. Regular exams are essential to detect common age-related conditions like glaucoma, cataracts, and macular degeneration. After age 65, annual eye exams are often recommended.
Choice B reason: You should have your hearing screened every 10 years, not every 5 years, until the age of 50. After 50, you should have a hearing test every 3 years.
Choice C reason:While stool-based testing for colorectal cancer (such as FOBT or FIT) is recommended starting at age 45, it is typically done annually, not every other year. Other screening methods, like a colonoscopy, may have a longer interval but should follow guidelines tailored to the patient’s risk profile.
Choice D reason: You should have your fasting blood glucose level checked every 3 years, not every 6 years, starting at age 45. This is a screening test for diabetes, which can increase your risk of heart disease, stroke, kidney disease, and other complications. If you have a history of gestational diabetes, obesity, or other risk factors, you may need more frequent testing.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today