A client has not voided eight hours after surgery and says to the nurse, “I don’t think I can urinate.” What should be the first action for the nurse?
Assess the client’s bladder.
Administer pain medication.
Increase the client’s fluid intake.
Inform the surgeon of the client’s status.
The Correct Answer is A
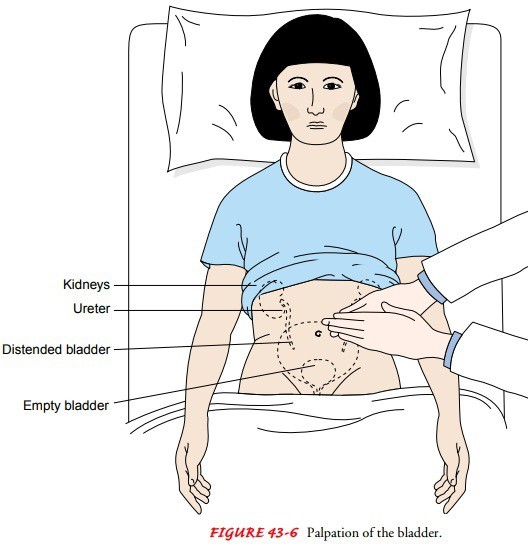
The nurse should first assess the client’s bladder for distention by palpating the lower abdomen between the symphysis pubis and the umbilicus.
This can indicate urinary retention, which is a common postoperative complication. The nurse should also measure the bladder volume using a bladder scanner if available.
Choice B. Inform the surgeon that the client’s status is wrong because the nurse should first assess the client before notifying the surgeon.
The surgeon may order interventions based on the assessment findings.
Choice C. Increasing the client’s fluid intake is wrong because increasing fluid intake may worsen bladder distention and discomfort.
The nurse should encourage fluid intake only after ensuring adequate urinary output.
Choice D. Administering pain medication is wrong because pain medication may not be indicated for urinary retention.
Pain medication may also cause urinary retention by relaxing the bladder muscles and impairing the micturition reflex.
Normal urine output is about 30 mL per hour or 240 mL in eight hours.
The nurse should monitor the client’s intake and output and report any signs of urinary retention to the surgeon.
Urinary retention can lead to infection, bladder damage, and renal impairment if not treated promptly.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
This is because a client who has been diaphoretic for the past six hours is likely to have wet and uncomfortable bed linens that can cause skin breakdown and infection. Changing the bed linens frequently can help keep the client dry and comfortable.
Choice A is wrong because offering the client a bedpan every three hours is not related to diaphoresis and may not meet the client’s elimination needs.
Choice B is wrong because keeping an emesis basin near the bedside is not related to diaphoresis and may not be necessary unless the client has nausea or vomiting.
Choice C is wrong because providing oral care every four hours is not enough to prevent dehydration and dry mouth in a client who has been diaphoretic for the past six hours. The client may need more frequent oral care and fluid intake.
Correct Answer is B
Explanation
This is because the resident is independent and sociable, and has the right to choose her own grooming preferences.
Serving her breakfast in her room will respect her autonomy and dignity, and prevent her from missing a meal.
Choice A is wrong because omitting her breakfast will deprive her of nutrition and hydration, and may cause health problems.
It will also violate her rights as a resident.
Choice C is wrong because getting her up early enough to be ready for breakfast will disrupt her sleep cycle and may cause fatigue or stress.
It will also impose the nurse’s values on the resident, and disregard her preferences.
Choice D is wrong because having her go to breakfast regardless of the state of her grooming will embarrass her and lower her self-esteem.
It will also disrespect her culture and values, and may affect her social interactions.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today