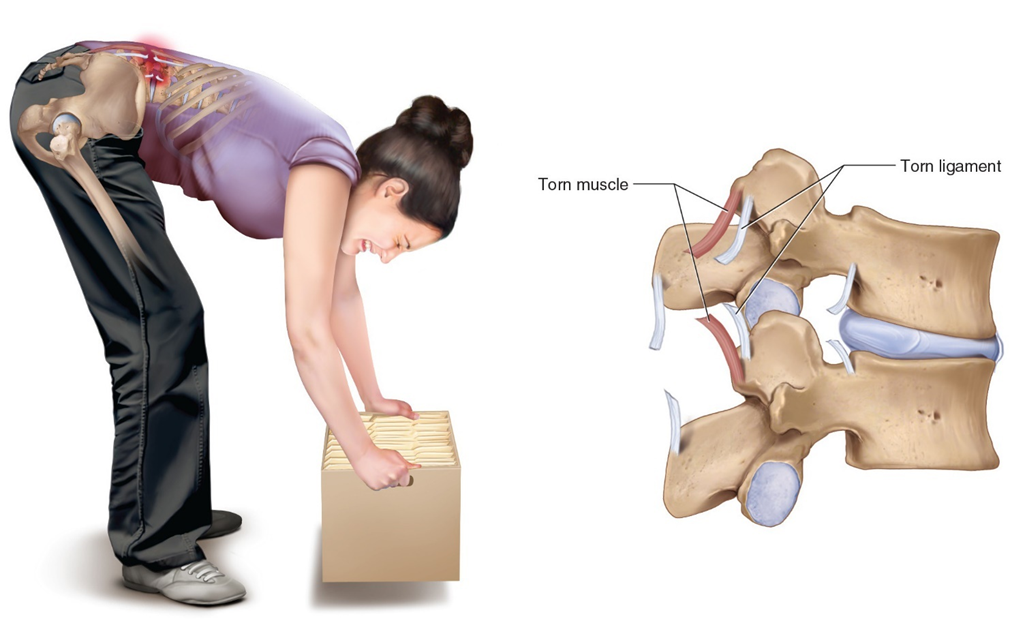
A heating pad is ordered for a patient with a lumbar sprain. The nurse knows that the purpose of the heating pad is to:
Promote healing by increasing the rate of the muscle remodeling process.
Decrease pain by reducing inflammation.
Decrease pain by increasing circulation to a painful area and relaxing tense muscles.
Decrease pain by numbing pain signals.
The Correct Answer is C
Choice A: Promote healing by increasing the rate of the muscle remodeling process
While heat can aid in the healing process by improving blood flow and nutrient delivery to the injured area, it does not specifically increase the rate of the muscle remodeling process. Muscle remodeling involves complex cellular activities that are not solely influenced by external heat application.
Choice B: Decrease pain by reducing inflammation
Heat therapy is generally not used to reduce inflammation. In fact, applying heat to an inflamed area can sometimes exacerbate the inflammation. Cold therapy is more effective for reducing inflammation, especially in the initial stages of an injury.
Choice C: Decrease pain by increasing circulation to a painful area and relaxing tense muscles
This is the correct answer. Applying heat to a painful area causes vasodilation, which increases blood flow and helps deliver oxygen and nutrients to the affected tissues. This process helps to relax tense muscles and alleviate pain. Heat therapy is particularly effective for muscle spasms, stiffness, and chronic pain conditions.
Choice D: Decrease pain by numbing pain signals
Heat therapy does not numb pain signals in the same way that cold therapy does. Cold therapy works by numbing the affected area and reducing nerve activity, which helps to alleviate pain. Heat therapy, on the other hand, works by improving circulation and relaxing muscles.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason:
Assessing the operative site is important to monitor for signs of bleeding, infection, or other complications. However, it is not the most critical, high-priority assessment immediately after surgery. While the condition of the surgical site can provide valuable information about the patient’s recovery and potential complications, it does not take precedence over ensuring the patient’s airway is clear and they are breathing adequately. The operative site can be assessed once the patient’s airway, breathing, and circulation are stable.
Choice B reason:
Airway assessment is the most critical, high-priority assessment in the PACU. Ensuring that the patient’s airway is clear and they are breathing properly is paramount because anesthesia can depress the central nervous system, leading to compromised airway patency and respiratory function. The primary goal in the immediate postoperative period is to ensure that the patient is ventilating adequately to prevent hypoxia and other respiratory complications. This involves checking for airway obstruction, monitoring respiratory rate, and ensuring that oxygen saturation levels are within normal ranges (typically 95-100% for healthy individuals). Any issues with the airway must be addressed immediately to prevent life-threatening complications.
Choice C reason:
Assessing the pulse is crucial for monitoring the patient’s cardiovascular status, including heart rate and rhythm. This can help detect arrhythmias, hypovolemia, or other cardiovascular issues that may arise postoperatively. However, while important, it is secondary to ensuring that the patient’s airway is clear and they are breathing adequately. The pulse can be assessed once the airway and breathing are confirmed to be stable. Normal pulse rates for adults typically range from 60 to 100 beats per minute.
Choice D reason:
Assessing skin integrity is important for identifying signs of pressure ulcers, infection, or other skin-related issues. However, this assessment is not the highest priority immediately after surgery. Ensuring the patient’s airway, breathing, and circulation are stable takes precedence. Skin integrity can be assessed once the patient is stable and other critical assessments have been completed. Maintaining skin integrity is essential for overall patient care, but it does not supersede the need to ensure the patient is breathing properly and has a clear airway.
Correct Answer is ["A","B","C","D","E"]
Explanation
Choice A: Collect patient information
The first step in the nursing process is to collect patient information, also known as the assessment phase. During this phase, the nurse gathers comprehensive data about the patient’s health status, including medical history, physical examination findings, and any relevant diagnostic test results. This information forms the foundation for identifying the patient’s needs and planning appropriate care.
Choice B: Identify any clinical problems
After collecting patient information, the next step is to identify any clinical problems, also known as the diagnosis phase. In this phase, the nurse analyzes the assessment data to determine the patient’s health issues or potential risks. This step involves critical thinking and clinical judgment to prioritize the patient’s problems and develop a nursing diagnosis.
Choice C: Decide a plan of action
The third step is to decide a plan of action, also known as the planning phase. During this phase, the nurse sets measurable and achievable goals for the patient’s care based on the identified clinical problems. The nurse also develops specific interventions to address these problems and achieve the desired outcomes. This plan serves as a guide for the subsequent implementation phase.
Choice D: Carry out the plan
The fourth step is to carry out the plan, also known as the implementation phase. In this phase, the nurse executes the planned interventions to address the patient’s clinical problems. This may involve administering medications, providing treatments, educating the patient and family, and coordinating care with other healthcare professionals. The nurse continuously monitors the patient’s response to the interventions and makes adjustments as needed.
Choice E: Determine whether the plan was effective
The final step is to determine whether the plan was effective, also known as the evaluation phase. During this phase, the nurse assesses the patient’s progress toward the established goals and evaluates the effectiveness of the interventions. If the desired outcomes are not achieved, the nurse may need to revise the plan and implement new strategies. This ongoing evaluation ensures that the patient’s care is continuously improved and optimized.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today